Winter 2025 Term
TITLE: PET Tracer [11C]-UCB-J as a Biomarker Enabling the Discovery of Targeted Therapeutics for Schizophrenia
INVESTIGATORS:
Jong Yoon (1)
Agnes Kalinowski (1)
Guido Davidzon (2)
Mehdi Khalighi (2)
(1) Department of Psychiatry
(2) Department of Radiology
DATE: Wednesday, 12 March 2025
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Schizophrenia (SZ) imposes significant economic and societal burdens due to lost productivity and the high cost of care, with U.S. annual costs estimated at $155.7 billion in 2013. Despite this impact, treatment remains limited to antipsychotics that target positive symptoms without addressing cognitive deficits, negative symptoms, or altering disease progression, leaving most individuals unable to achieve stable employment and requiring lifelong support. Progress in developing novel treatments is hindered by the heterogeneity of schizophrenia and the limitations of the current symptom-based diagnostic system, which groups cases with disparate underlying pathologies. Advances in biomarker development, particularly the use of 11C-UCB-J PET imaging, the first-in-human in vivo synapse marker to measure synaptic density, offer hope for refining subject selection and improving clinical trial outcomes. Synaptic density deficits, linked to mechanisms like excess synaptic pruning mediated by complement 4 protein pathways, are emerging as a common pathway in some schizophrenia subgroups. 11C-UCB-J has been validated as a reliable in vivo synapse marker and shows promise as both a subject selection biomarker to reduce heterogeneity and a response biomarker for evaluating treatments targeting synaptic pathology. This approach could facilitate the discovery of novel therapies for schizophrenia, leveraging ongoing trials of agents targeting synaptic elimination pathways.
HYPOTHESIS & AIM
To develop 11C-UCB-J PET imaging as a biomarker aiding in the selection of case of schizophrenia with synaptic deficits for clinical trials testing the effectiveness agents targeting cognitive deficits arising from synaptic pathology. We hypothesize that these selected cases will respond favorably to treatment compared to controls.
DATASET
We completed 11C-UCB-J PET scans on 18 healthy individuals and 25 individuals with SZ. These subjects have also undergone characterization of their cognitive abilities using the Brief Assessment of Cognition in Schizophrenia (BACS), a brief, highly reliable, cognitive battery measuring six cognitive domains, as well as their level of psychopathology.
STATISTICAL MODELS
To be determined.
STATISTICAL QUESTIONS
- What are methods or models are recommended for identifying subset or cluster of SZ subjects with synaptic deficits?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
DATE: Wednesday, 5 March 2025
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
TITLE: Accounting For Sex-Linked Variation: A Machine Learning-Generated Index for Assessing Abdominal Aortic Aneurysm Rupture Risk and Progression
INVESTIGATORS:
Lauren Aalami (1)
Elizabeth George (2)
Akshay Chaudhari (3, 4)
- Department of Radiology
- Department of Vascular Surgery
- Department of Radiology
- Center for Artificial Intelligence in Medicine & Imaging (AIMI)
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Ruptured abdominal aortic aneurysms (AAAs) are the 13th leading cause of death in the United States, causing an estimated 15,000 deaths per year. AAAs are generally asymptomatic prior to rupturing, at which point mortality is 85–90%, making predictive and proactive AAA screening, monitoring, and rupture risk assessment crucial. Today, the most widely used and robustly validated criterion for defining/diagnosing abdominal aortic aneurysms (AAAs), assessing AAA rupture risk, and choosing when to operate is maximal AAA diameter–the width of the aneurysmal aorta at its widest point. The problem with using this metric as an expression of AAA progression and rupture risk, however, is that maximal AAA diameter alone cannot account for human variation in baseline/healthy aortic diameter. One universally-applied operative threshold assumes one universal baseline aortic diameter, which is not reflected in human anatomy, and even sex-specific diameter-based thresholds assume that every woman has a smaller healthy/normal aortic diameter than every man, which is not the case.
HYPOTHESIS & AIM
Prior works (Ouriel et al.) indicate that standardization of the aneurysm diameter to the transverse diameter of the third lumbar vertebral body (L3) as an index of patient body size may produce a more accurate predictor of rupture than raw aneurysm diameter alone. This promising alternative to diameter-only AAA rupture-risk assessment has gone untested and unimplemented for more than 30 years, likely in part due to the logistical burden associated with manual index calculation. The goal of this project is to create a machine learning Picture Archiving and Communication System (PACS) plug-in that automatically generates a ratio of maximal aortic diameter relative to the transverse diameter of L3 on abdomen/pelvis computed tomography (CT) scans—a measure of AAA progression/rupture risk that accounts for baseline variation in body habitus and normal aortic diameter in a way that diameter alone does not.
DATASET
Internal training and validation datasets will be comprised of approximately 25K abdomen and pelvis CT scans (CPT codes 72192, 72193, 72194, 74150, 74160, 74170, 74176, 74177, and 74178) identified via the STAnford Research Repository (STARR) tool. Corresponding radiologic reports and ICD codes assigned during the encounter are also to be pulled.
STATISTICAL QUESTIONS
What statistical methods should we employ in order to:
- Capture the influence of diagnostic criteria (3.0 cm diagnostic threshold, ASI, etc.) on the incidence of AAAs within our dataset?
- Identify the index value (the actual ratio) that is predictive of a diagnosed AAA within our dataset? In other words: what index value/cutoff corresponds to the point at which AAAs are diagnosed; both within patient records (ICD codes) and using the various AAA definitions (3.0 cm, ASI, etc.).
- Determine how well the index (using Ouriel’s 1.0 ratio, or the ratio that we judge best) stratifies ruptured from unruptured aneurysms? In other words: determine which method of expressing aneurysm size is the best discriminator of aneurysm rupture?
- Create a risk stratification chart (annual aneurysm rupture at increasing index values) to assist in clinical decision making?
- Determine the index value that best stratifies ruptured from unruptured AAAs in our dataset?
- Identify a new index-based operative threshold?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
—
TITLE: An Exploratory Naturalistic Analysis of Daily Frequency of Transcranial Magnetic Stimulation Treatment
DATE: Wednesday, 26 February 2025
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
INVESTIGATORS:
Alisa Olmsted (1,2)
Jong Yoon (1,2)
- Veterans Affairs Palo Alto Healthcare System, and the Sierra Pacific Mental Illness, Research, Education, and Clinical Center (MIRECC), Palo Alto, CA
- Department of Psychiatry and Behavioral Sciences, Stanford University Medical Center, Stanford, CA
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Major depressive disorder (MDD) is a chronic, debilitating condition that affects 24.9% of the U.S. population during their lifetime. Of those diagnosed, approximately 35% experience treatment-resistant depression (TRD), characterized by a lack of response to at least two adequate antidepressant trials. Transcranial Magnetic Stimulation (TMS) is a non-invasive neuromodulation treatment for TRD approved by the FDA in 2008, in which an electromagnetic coil delivers repetitive pulses to modulate cortical activity and neural excitability. In the Veteran population, once-daily 10 Hz TMS over 4–6 weeks has been shown to be clinically effective for MDD. Intermittent theta burst stimulation (iTBS), a 50 Hz variation of TMS, has been demonstrated to be non-inferior to 10 Hz protocols while significantly reducing treatment time to just minutes. More recently, the FDA-approved SAINT protocol, which administers 10 sessions of iTBS per day over five days, has highlighted the potential of multiple treatments daily for rapid symptom relief in select populations. As clinics increasingly adopt accelerated protocols with more than once daily treatment, research on the efficacy and optimization of these approaches remains limited.
HYPOTHESIS & AIMS
Aim 1: To demonstrate clinical outcomes in TMS for TRD are primarily driven by cumulative stimulation dose, rather than the specific protocol or the number of sessions administered per day.
Hypothesis 1a: 10 Hz and iTBS stimulation are equivalent in the reduction of depressive symptoms.
Hypothesis 1b: Increasing daily frequency of treatment will impact outcomes as a reflection of cumulative stimulation delivered rather than a specific treatment schedule.
Aim 2: To estimate the number of additional treatments needed in delayed responders.
Hypothesis 2: Delayed responders will demonstrate a sigmoid dose-response with additional cumulative stimulation needed to reach benefit.
STUDY CHARACTERISTICS
This secondary analysis, part of a larger quality improvement study, examines the clinical effects of TMS in Veterans. Eligible Veterans received TMS at the Precision Neuromodulation Clinic (PNC) at VA Palo Alto between September 2017 and February 2025. Eligibility was determined by a psychiatrist based on FDA guidelines for MDD, including prior medication resistance and moderate functional impairment. Exclusion criteria included bipolar disorder, borderline personality disorder, cardiac or seizure risks, and metal implants in the head/neck.
Veterans underwent motor threshold (MT) assessment using the Beam F3 method and the PEST program, with treatment delivered at 120% MT using a MagStim Horizon or Rapid2 figure-of-8 coil. The standard protocol included 30 sessions, adjusted based on clinical response and tolerability. Depression severity (PHQ-9) was assessed at baseline and weekly throughout treatment. Veterans were excluded if pre/post PHQ-9 data were unavailable or if baseline PHQ-9 scores were ≤5, indicating minimal depression.
STATISTICAL MODELS
The primary outcome was PHQ-9 change from baseline to post-treatment over the course of TMS. Cumulative stimulation was calculated as a weighted sum of the number of treatment sessions times the percent MT the treatment was delivered. Treatments were targeted at 120% MT, but if administered at 90% MT for example, a weight of 0.9 was assigned for that session. If multiple MT values were recorded, the percent MT was recalculated accordingly for subsequent days.
The number of treatments delivered was analyzed in two ways: 1) final session count recorded in the national database, and 2) adjusted session count. This was calculated as total clinic days from treatment start to end divided by the total number of sessions received. This method accounted for missed treatment days.
To control for baseline variability, ANCOVA-adjusted post-treatment PHQ-9 scores, with baseline PHQ-9 as a covariate. PHQ-9 change from baseline was analyzed across groups based on daily treatment frequency. Treatment courses were modeled by week and by cumulative stimulation delivered, then evaluated qualitatively.
STATISTICAL QUESTIONS
(1) How should we compare the effectiveness of 10Hz vs. iTBS in this naturalistic dataset?
(2) How should I summarize my data?
(3) What is the best way to model treatment response across different treatment schedules with varying numbers of treatment sessions daily?
(4) How can we estimate the number of additional treatments needed for delayed responders?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
DATE: Wednesday, 19 February 2025
TIME: 3:00–4:30 PM
TITLE: Efficiency and power in clinical trials using biomarkers and genetic risk scores
INVESTIGATOR:
Manuel A. Rivas, Department of Biomedical Data Science
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
The incorporation of biomarkers into clinical trials has the potential to improve trial efficiency, reduce required sample sizes, and increase statistical power to detect treatment effects. By identifying and measuring reliable biomarkers early in the trial, researchers can refine patient selection, stratify risk, and potentially replace or supplement traditional endpoints with more responsive or biologically relevant measures. Despite these advantages, questions remain regarding the appropriate study design, analysis plan, and methodological strategies to ensure that incorporating biomarkers truly enhances the power of a trial rather than inflating Type I error or introducing bias.
In this project, we explore how biomarker-driven clinical trial designs can efficiently allocate resources while retaining high power to detect meaningful differences in treatment outcomes. We will illustrate these ideas with cardiovascular disease clinical trials that includes biomarker measurements and polygenic risk scores.
HYPOTHESIS & AIM
We hypothesize that using biomarkers as intermediate or surrogate endpoints in clinical trials can (1) reduce the necessary sample size to achieve desired power and (2) more accurately predict treatment effects on long-term clinical outcomes. Specifically, we aim to:
- Compare the power and sample size requirements for standard trial designs versus biomarker-enriched designs.
- Investigate how early biomarker changes correlate with final clinical outcomes, and whether these relationships can be leveraged for adaptive trial modifications.
- Develop statistical models that incorporate continuous and categorical biomarker data to enhance endpoint sensitivity and specificity.
DATASET
We plan to simulate data for clinical trial design using biomarker measurements obtained in population biobanks like UK Biobank and genetic risk scores.
STATISTICAL MODELS
We will investigate classical approaches to modeling biomarker trajectories and linking them to clinical outcomes. Our plan includes Adaptive Design Simulations to explore how real-time biomarker data might trigger modifications to sample size or randomization schemes.
STATISTICAL QUESTIONS
- Optimal Endpoint Selection
- How do we determine which biomarkers are most predictive of meaningful clinical outcomes?
- What statistical criteria should guide the choice of a biomarker-based surrogate endpoint?
- Sample Size & Power
- How can we quantify reductions in required sample size when using biomarker enrichment?
- What methodologies (e.g., simulation-based power calculations) are appropriate to assess these potential gains?
- Modeling Strategy
- When should we incorporate biomarkers as fixed covariates versus time-varying covariates?
- How do we handle missing biomarker data or measurement error over repeated timepoints?
- Adaptive Designs
- Can early biomarker changes be used to modify enrollment or randomization mid-trial without inflating Type I error?
- What practical and regulatory considerations arise when using interim biomarker data to adapt the trial?
- Validation & Generalizability
- How do we validate biomarker-based endpoints across diverse patient populations and multiple centers?
- Are there standard metrics or thresholds that help establish external validity for biomarker-driven findings?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
DATE: Wednesday, 12 February 2025
TITLE: Data Studio Office Hour
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
ZOOM MEETING INFORMATION:
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
DATE: Wednesday, 22 January 2025
TITLE: Data Studio Office Hour
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
ZOOM MEETING INFORMATION:
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
TITLE: Data Studio Office Hour
DATE: Wednesday, 15 January 2025
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
ZOOM MEETING INFORMATION:
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
TITLE: Data Studio Kickoff Meeting
DATE: Wednesday, 8 January 2025
TIME: 3:00–4:30 PM
LOCATION: Conference Room R318, Edwards Building, 300 Pasteur Drive, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
AGENDA
The first session of Data Studio for this quarter, also available as BMDS 291 for students, will include faculty-student introductions, a review of the course syllabus, and an introductory lecture about the art of data science consultation. If you wish to learn more, you are welcome to attend in-person.
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/94651266419?pwd=c8sogIr0LEdQzvHgsPdmvm6s9IXnsr.1
Meeting ID: 946 5126 6419
Password: 846732
Or iPhone one-tap (US Toll):
Password: 846732
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 946 5126 6419
Password: 846732
Password: 846732
Fall Term 2024
TITLE: Evaluating Mineralocorticoid Receptor Antagonist Responsiveness in the SPRINT Cohort
INVESTIGATORS:
Jia Wei Tan (1)
Vivek Bhalla (1)
Manjula K. Tamura (1,2)
(1) Stanford University School of Medicine, Department of Nephrology
(2) VA Palo Alto Geriatric Research Education and Clinical Center
DATE: Wednesday, 4 December 2024
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
African Americans (AA) may retain more sodium than Caucasians, leading to suppressed renin and aldosterone secretion. The epithelial sodium channel (ENaC), which regulates sodium reabsorption, might have differing activity levels in AAs, contributing to sodium retention or reduced aldosterone stimulation. The RALES study found that spironolactone was less likely to cause hyperkalemia and less effective in reducing death or heart failure hospitalizations in AAs compared to Caucasians, indicating a potential racial difference in its clinical outcomes. Genetic differences, such as the CYP4A11 rs3890011 CC genotype, may play a role, as this genotype is associated with blood pressure resistance to mineralocorticoid receptor antagonists (MRAs) but sensitivity to ENaC inhibition. Variants in the mineralocorticoid receptor (NR3C2) gene, like the c.-2C>G (rs2070951) polymorphism, occur more frequently in Caucasians than in AAs, raising the possibility that genetic variants of NR3C2 could influence clinical outcomes. This study seeks to evaluate racial differences in responsiveness to MRAs to understand these disparities better.
HYPOTHESIS & AIM
We propose using changes in systolic blood pressure (ΔSBP) before and after MRA treatment as a surrogate marker for MRA responsiveness. Our hypotheses as below:
1) The change in systolic blood pressure following MRA treatment in Caucasians is different compared with African Americans.
2) The change in serum potassium following MRA treatment is greater in Caucasians than African Americans.
3) The change in systolic blood pressure following MRA treatment depends on baseline serum potassium levels. After MRA treatment, Caucasians with lower baseline serum potassium levels do not show a greater reduction (i.e., less than or equal to) in SBP than African Americans with lower baseline serum potassium levels.
DATASET
We used data from the SPRINT (Systolic Blood Pressure Intervention Trial) dataset, a large, randomized, controlled, open-label trial conducted across 102 clinical sites in the United States. SPRINT was designed to test whether lowering systolic blood pressure (SBP) to below 120 mm Hg, as compared to a target of below 140 mm Hg, would reduce cardiovascular events and mortality. The trial included participants aged 50 and older, with an SBP between 130 and 180 mm Hg and an elevated cardiovascular disease (CVD) risk (e.g., clinical or subclinical CVD, chronic kidney disease, or high Framingham risk score). Patients with diabetes or a history of stroke were excluded. A total of 9361 participants were enrolled, split almost evenly between a standard treatment arm (target <140 mm Hg) and an intensive treatment arm (target <120 mm Hg). Given its early termination after a median follow-up of 3.26 years, the study found significant benefits of intensive SBP reduction, with a 25% reduction in CVD events and a 27% reduction in all-cause mortality. From this dataset, I analyzed 329 MRA users and 1530 Thiazide users to investigate outcomes related to aldosterone sensitivity in these treatment groups.
STATISTICAL MODELS
We used a student’s t-test (two-sided) to evaluate the SBP response to MRA treatment. We used continuous SBP change initially to avoid arbitrary cutoffs, and then used quantile regression to predict SBP response to MRA treatment. We used the 25th and 50th percentile to categorize the research subjects as “good responders,” while controlling for various covariates including BMI, treatment assignment, age, gender, race, CKD status, and cardiovascular disease history. We also used a multiple linear regression model using ordinary least squares (OLS) to examine the relationship between potassium changes and systolic blood pressure changes, while controlling for various covariates as stated before. Separate regression lines were fitted for Black and non-Black participants to assess potential racial differences in the relationship between potassium and blood pressure changes. The models included the calculation of 95% confidence intervals and p-values to assess the statistical significance of the relationships, with visual representation through partial regression plots showing both the individual data points and fitted regression lines. The analysis also included diagnostic statistics such as R-squared values to assess model fit and coefficient values to quantify the strength and direction of relationships.
STATISTICAL QUESTIONS
(1) What is the best method to define “responders?” (linear regression or quantile regression?)
(2) What statistical approach should be used to account for potential confounding variables (such as intensive versus standard treatment assignment) while maintaining sufficient statistical power, given the relatively small sample size of MRA users (n=329)?
(3) How should we model the interaction between race and baseline potassium levels to test hypothesis #3 (whether Caucasians with lower baseline potassium levels show different SBP reductions compared to African Americans)?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
There is no Data Studio session during the week of 25–29 November in observance of the Thanksgiving Holiday.
DATE: Wednesday, 20 November 2024
TITLE: Data Studio Office Hour
DATE: Wednesday, 20 November 2024
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
ZOOM MEETING INFORMATION:
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 13 November 2024
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
TITLE: Phase I Clinical Trial Design of GPC2-Targeted CAR T-Cell Therapy for Relapsed/Refractory Medulloblastoma and ETMR in Children and Young Adults
INVESTIGATORS:
Edward (Dehua) Bi (Presenter; 1)
Sabine Heitzeneder (Presenter; 2)
Katie J. Ryan (2)
- Stanford Cancer Institute
- Pediatrics/Hematology-Oncology
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Pediatric medulloblastoma is the most common malignant brain tumor in children, with a five-year overall survival rate of around 80% for standard-risk cases. However, relapsed and refractory medulloblastoma (RR-medullo) remains a major challenge, affecting 25–30% of patients and offering a poor prognosis with survival rates as low as 10%, despite repeated surgeries and re-irradiation. Embryonal tumor with multilayered rosettes (ETMR), another aggressive pediatric brain tumor, primarily impacts children under five and has a similarly bleak outlook, with survival rates below 30% despite aggressive treatment. These statistics underscore an urgent need for more effective and targeted therapies for children with high-risk medulloblastoma and ETMR.
Chimeric antigen receptor (CAR) T-cell therapy is an emerging immunotherapy that reprograms a patient’s own T-cells to target specific tumor markers. In this trial, glypican-2 (GPC2), a protein highly expressed in medulloblastoma and other central nervous system tumors, has been selected as the target for CAR T-cell therapy. CAR T-cells engineered to recognize GPC2 are intended to specifically attack cancer cells, sparing healthy tissue. This Phase I trial will evaluate the feasibility of manufacturing CAR T-cells targeting GPC2 and assess the safety and tolerability of this novel approach in children and young adults with aggressive brain tumors.
TRIAL OBJECTIVES
We want to design a Phase I clinical trial for children and young adults with RR-medullo or embryonal tumor with multilayered rosettes (ETMR). There are two primary objectives:
- Determine the feasibility of manufacturing autologous T-cells transduced with a GPC2 retroviral vector to express anti-GPC2 CAR T-cells.
- Assess the safety and describe toxicities associated with intracerebroventricular (ICV) administration of GPC2-CAR T-cells utilizing a protocol-directed dose escalation schedule to carefully monitor and escalate doses.
TRIAL REQUIREMENTS
We define feasibility as the consistent production of GPC2-CAR T-cells that meet minimum standards for transduction efficiency, cell yield, viability, and all IND release criteria with an acceptable success rate across multiple manufacturing batches.
The trial involves dose selection based on the following GPC2-CAR T-cell dose levels (±20%, non-weight-based):
Table 1 Dose levels of anti-GPC2 CAR T-cells. All patients will start at ICV DL 1.
| ICV Dose Levels (DLs) | Dose of Transduced T-cells ±20%, non-weight-based. |
| ICV DL -1 | 5×106 |
| ICV DL 1 | 10×106 |
| ICV DL 2 | 30×106 |
| ICV DL 3 (potentially remove this level) | 50×106 |
Prior to the initial CAR T-cell infusion at ICV DL 1, all patients will undergo LD. Following this, CD4 T-cell counts will be monitored every 3 months. If a patient’s CD4 T-cell count falls below a specified threshold, LD will be performed again before the next cycle of CAR T-cell infusion. We anticipate that LD followed by the first CAR T-cell infusion may induce higher toxicity compared to LD followed by any dose level in subsequent treatment cycles. Therefore, the dose for Cycle 1 will be capped at ICV DL 1. For subsequent cycles, dose levels above ICV DL 1 may be permitted following LD.
CLINICAL TRIAL DESIGN
The clinical trial parameters are a target toxicity rate of 30%, a maximum of 8 treatment cycles, and a maximum sample size of 12 patients. We are considering an intrapatient dose escalation design because patients will undergo multiple treatment cycles. We plan to use an Accelerated Titration (AT) design that transitions to the i3+3 design to evaluate safety. This intrapatient dose-escalation approach determines dose levels for both newly-enrolled patients in their first treatment cycle and currently-enrolled patients in their subsequent cycles based on accumulated patient data.
All patients will receive LD prior to their first CAR T-cell infusion, no matter the dose level. During the AT phase, patients will begin their first treatment cycle at ICV DL 1. If no dose-limiting toxicity (DLT) occurs during Cycle 1, the patient will be escalated to ICV DL 2 for Cycle 2. If no DLT occurs during Cycle 2, the patient will be escalated to ICV DL 3 for Cycle 3. The patient will remain at ICV DL 3 for subsequent cycles as long as no DLT is observed. This dosing schedule will be applied to all patients until a DLT is observed in any cycle for any patient. The occurrence of a DLT will then trigger a switch from the AT design to the i3+3 design.
The i3+3 clinical trial design guides dose level selection decisions by comparing the observed DLT rate at a given dose level to an equivalence interval (EI) of toxicity probabilities centered around the target toxicity. For example, if the target toxicity is 30%, an EI of [0.25, 0.35] implies that toxicity rates within this range are equivalent to the target. Based on this comparison, the following decisions can be made for the next cohort of patients.
- Escalate (E): Increase to the next higher dose level.
- Stay (S): Maintain the same dose level.
- De-escalate (D): Decrease to the next lower dose level.
Using this design for intrapatient dose level selection, we will apply the standard i3+3 framework to determine whether to de-escalate to ICV DL -1 or remain at ICV DL 1 for new patients entering Cycle 1. This decision will be based on the observed DLT rate among all patients treated at ICV DL 1 during Cycle 1. For subsequent treatment cycles of each currently enrolled patient, we will apply the following rules for dose level selection based on whether or not the patient experienced a DLT in the previous cycle.
- If a DLT occurred in the patient’s previous cycle: Their dose level will automatically be de-escalated, unless the patient was already at dose level ICV DL -1, in which case the patient will remain on that dose level.
- If no DLT occurred in the patient’s revious cycle: The dose level for the next cycle will be determined based on all accumulated patient data of that dose level (?) from cycles 1 through the current cycle.
At the end of the trial, we will tabulate the frequency of toxicities (estimated toxicity rate) for each dose level within each cycle as well as cumulatively across cycles to develop a comprehensive toxicity profile of the treatment. We are currently exploring strategies for selecting the most promising sequence of dose levels to identify the MTD or RP2D sequence.
STATISTICAL QUESTIONS
We have the following statistical questions regarding the design.
- What is an acceptable success rate for the feasibility of manufacturing GPC2-CAR T-cells?
- How do we incorporate feasibility success rate into the trial design?
- Is the design appropriate to address the second objective of the trial?
- What strategies could be employed to select the best sequence of dosing/most tolerable sequence of dosing? The complication here is that each patient may have different length of treatment and a different sequence of dosing which implies that there might be no or only a few sequences that have a count greater than 1. In this case, how can we find the best sequence of dosing?
- We anticipate that the first cycle of CAR T-cell ICV infusion with LD is the most toxic one. That is why the clinical team does not want to try LD with a DL greater than ICV DL 1 for the first infusion. However, for subsequent cycles, we believe that LD plus other CAR T-cell dose levels will not evoke as much toxicity. Furthermore, we also believe that LD plus any dose level of CAR T-cells has a higher toxicity level than these dose levels without LD. Given that LD during subsequent treatment cycles will be administered based on CD4 counts, what are possible ways to incorporate this LD schedule into the trial design?
- Based on a previous trial with GD2-CAR T-cells, each patient’s tolerance depends on tumor location, where they are on the path to progression (this is a fast-moving disease), how the patient responds, and other drugs they may be on while undergoing the interventional therapy. The investigators want to stay on the same dose when it’s been tolerated on a case-by-case basis. However, the problem is that if the patient is able to stay at the current dose level from a previous cycle, the next decision needs to be guided by data from all patients. We believe that the only possibility for dose level de-escalation is when there are multiple DLTs observed on the dose level that is assigned to the patient in previous cycle of treatment. Is variability the only way that the patient is able to stay at the current dose level?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
+18333021536,,93494617954# or
+16507249799,,93494617954#
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
SIP: 93494617954@zoomcrc.com
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 6 November 2024
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
TITLE: Research Participant Engagement Program (PEP): Program and Metrics Evaluation
INVESTIGATORS:
Andrea Bolanos (1)
Katherine Connors (1)
Maya Berdichesky (1)
Anisha Patel (2)
Tina Hernandez-Boussard (3)
- Stanford Center for Clinical and Translational Research and Education
- Division of General Pediatrics, Department of Pediatrics
- Biomedical Informatics Research, Department of Medicine
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
TITLE: Research Participant Engagement Program (PEP): Program and Metrics Evaluation
INTRODUCTION
Participant recruitment is among the most significant challenges faced in successful clinical research. The Research Participant Engagement Program (PEP) aims to assist study teams in achieving their recruitment goals by providing a variety of resources. These services include Direct Email outreach, notifications through Epic (Children’s) MyChart, Epic (Adult) MyHealth, Postal Mail, and outreach via the Stanford Research Registry. To ensure the continued effectiveness and relevance of our program, we would like to conduct a comprehensive program evaluation. This evaluation will allow us to assess our strengths and weaknesses, identify areas for improvement, and strategize for the future roadmap of PEP.
HYPOTHESIS & AIM
We hypothesize that studies yield higher interest from potential participants, if:
- Comprehension: the study invitation has high readability (e.g. 8th grade reading level or below)
- Compensation: the study has high compensation (monetary, but also benefits such as receiving free health information) — how to quantify?
- Commitment: the study has low time commitment — how to quantify? Also, interested in time commitment:compensation ratio
- Criteria: the study has simple eligibility (fewer inclusion/exclusion criteria)
We are calling these the 4 Cs: Comprehension, Compensation, Commitment, Criteria. The purpose of this evaluation is to identify trends and common benchmarks as well as more knowledge on expected interest rates. Our Inclusive Participation tool is aimed at increasing diverse representation in research. We are seeking statistical expertise on how to appropriately implement this tool, accounting for sampling bias or other concerns.
DATASET
The study will be looking at the data pulled from our PEP Platform. By gathering insights from both our metrics and study teams, we aim to understand why we see such a wide range in our % interested metrics. We will be comparing the following categories between the 4 studies with the highest % interested participants and the 4 studies with the lowest % interested – using the 4Cs: comprehension, compensation, commitment, and criteria.
| Outreach Channel | # Studies | # Invitations | # Interested | % Interested | % Interested Range | Date Launched |
| Direct Email | 22 | 227,804 | 3,389 | 1.5% | 0.2 – 7.7% | Feb 2020 |
| Epic MyChart | 37 | 123,881 | 2,561 | 2.1% | 0.0 – 21.4% | Mar 2020 |
| Epic MyHealth* | 19 | 147,823 | 852 | 0.6% | 0.0 – 10.3% | Sep 2022 |
| Postal Mail | 25 | 59,724 | 267 | 0.4% | 0.0 – 31.6% | May 2020 |
| PEP Total | 72 (unique studies) | 559,232 | 7,069 | 1.3% | ||
| Children’s Epic BPAs | 3 | 5,805 | 1,444 | 24.9% | 22.8 – 38.5% | May 2020 |
| Stanford Research Registry | 43 | 44,028 | 4,299 | 9.8% | 0.2 – 66.7% | Apr 2020 |
| SRR- not COVID related | 38 | 37,064 | 1,980 | 5.3% | ||
| SRR- COVID related | 5 | 6,964 | 2,319 | 33.3% | ||
| StudyPages (active or finished) | 122 | Views/Clicks: | Sign-ups: | Of Views: | Jan 2018 | |
| 361,826/20,659 | 16,640 | 4.6% |
Table 1 Data pulled from our PEP Platform.
STATISTICAL MODELS
Our PEP Platform now has a new tool, known as Inclusive Participation. The tool allows us to tailor our recruitment outreach by Race, Ethnicity, and Sex categories. While considering the goals of the study, we can use this tool to increase outreach to underrepresented groups. The Inclusive Participation tool is displayed below for a study prioritizing non-white participants:
Figure 1 Across all 3 categories at the same time, the Platform will prioritize by Ranking order. Benchmark % is based on Bay Area census, and the Target Population % is what we can edit.
STATISTICAL QUESTIONS
We are seeking help on what statistical model to use to test our hypothesis.
- Does it make sense to take the 4 top and 4 bottom from our metrics table?
- How will we compare/create benchmarks for the 4Cs?
- What are the statistically sound default settings for the Inclusive Participation tool?
- A question about Inclusive Participation tool: “If Latino is prioritized for Ethnicity, how long will it take to get to (non-Latino) Black/African American for Race?”
- How do we address sampling bias?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 30 October 2024
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
TITLE: Predicting Demographics and Clinical Values with Omics Data
INVESTIGATORS:
Daniel J. Panyard (1)
Tejaswini Mishri (1)
Hirotaka Ieki (1)
Aubrey Roberts (1)
Martín Acosta Parra (1)
Michael Snyder (1)
(1) Department of Genetics
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Multiomics analysis (transcriptomics, proteomics, metabolomics, etc.) is becoming widespread in the study of disease and human health as the amount of data collected can provide necessary insights into complex biological processes underlying a biological question. To this end, our lab conducted The Integrated Personal Omics Profiling (IPOP) and conducted multiomics analysis with the goal of revealing new insights in type 2 diabetes mellitus (T2D). The longitudinal dataset has been the subject of several follow-up analyses in the areas of glucose dysregulation, aging, and precision medicine. However, these analyses and others conducted on similar datasets have focused on characterizing “disordered” subjects from some “control” even though there is not a universally recognized “baseline” for omics data.
HYPOTHESIS & AIM
In this follow-up analysis, we want to lay out best practices for researcher beginning to work with large, longitudinal multiomics datasets to establish a “baseline” which would complement analyses focusing on variations from baseline. We aim to 1) quantify molecular variation in a “typical” population and identify molecular features associated with 2) demographics (sex, age, BMI), and 3) clinical tests. We hope that these analyses act as a resource for the growing multiomics community and aids in maximizing the use of these large datasets while minimizing complications from internal variability.
DATASET
The iPOP (Integrated Personal Omics Profiling) study is a longitudinal study of approximately 100 individuals meant to help lay a foundation for precision personalized medicine through the unprecedented deep biochemical profiling of generally healthy individuals. A significant portion of the cohort is pre-diabetic. We have multiomics analyses (transcriptomics, metabolomics, proteomics, microbiome data, cytokines, and clinical tests) for all these subjects but only a subset have all data collected (94 subjects). For those subjects which have all -omics data, we have heterogeneity in terms of number of visits, time between visits, and demographic distribution (the dataset is enriched for Caucasian and Asian individuals).
STATISTICAL MODELS
We are specifically interested in machine learning models to work with longitudinal data. At the outset, we have started our analyses using both standard logistic regression and random forest models. We are also developing a workflow using R/tidymodels to test several different ML models. However, we are mainly coming to Data Studio seeking advice on best practices modeling longitudinal data and ML model recommendations.
STATISTICAL QUESTIONS
- Longitudinal analysis—how to handle having multiple rows/visits per person?
- If/how we should down-sample individuals to avoid bias toward those with more visits?
- Any issue if the folds are slightly different sample sizes?
- How many folds to use in cross-validation?
- Train/test splitting by race/ethnicity with very uneven distribution?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 23 October 2024
TIME: 3:00–4:30 PM
TITLE: Assessing the Influence of Female Department Chairs on Female Representation Among General Surgery Residents
INVESTIGATORS:
Alexander Ren (1)
Jeff Choi (1)
Sherry Wren (1,2)
(1) Department of Surgery, Stanford University
(2) Department of General Surgery, VA Palo Alto Health Care System
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION:
While female representation among general surgery residents continues to climb, leadership in academic surgery remains largely male-dominated.1 Research has shown that female surgical role models are critical for the recruitment and retention of female surgery residents.2 Santosa et al. found that higher female representation among the faculty at surgical training programs is significantly associated with higher female representation among program residents.3 Furthermore, a cross-sectional study of plastic surgery residency programs found that programs led by a female chair were associated with a 45% relative increase in the proportion of female residents, but this association was not statistically significant.4 It remains unclear whether female chairs of general surgery departments have a direct effect on the gender composition of resident classes.
HYPOTHESIS & AIM:
We hypothesize that female representation among entering general surgery resident entrants increases in the classes following the appointment of a female academic department chair.
DATASET:
Female chairs of academic general surgery departments were identified using the roster presented on the website of the Association of Women Surgeons in the first quarter of 2023. The date of chair appointment was determined as precisely as possible through Google searches for relevant press releases. Female chairs were included in our analysis if (1) their department maintains an accredited categorical general surgery residency program, (2) there are at least 6 years of entering resident classes following their appointment and during their tenure as chair, (3) the immediate preceding chair was male, and (4) the chair was appointed prior to 6/7/2018 and after 3/18/2005, such that there is sufficient GME Track/ERAS data available for our analysis. We identified 14 female-led departments as well as 28 male-led departments (2:1 matched on geographical location [i.e. nearest male-led programs] across the same ten-year range). We then purchased a data set from the AAMC with the following information for the 42 programs of interest. For each program, we obtained the number of categorical general surgery resident entrants and applicants in each of the five years pre- and post-female chair appointment. This count data is stratified by sex and race/ethnicity.
STATISTICS:
Based on the date of appointment, we will conduct a differences-in-differences analysis comparing female-led and matching male-led programs in terms of the gender compositions of the five resident classes immediately prior to chair appointment and the five classes post-appointment.
STATISTICAL QUESTIONS:
(1) In addition to a difference-in-differences analysis looking at gender composition, what are additional analyses that could be interesting to explore using our custom dataset?
(2) Are there additional features of our programs-of-interest that could be useful for stratifying our data for subgroup analysis?
REFERENCES:
- Cochran A, Freischlag JA, Numann P. Women, Surgery, and Leadership: Where We Have Been, Where We Are, Where We Are Going. JAMA Surgery. 2013;148(4):312-313. doi:10.1001/jamasurg.2013.1706
- Neumayer L, Kaiser S, Anderson K, et al. Perceptions of women medical students and their influence on career choice. Am J Surg. 2002;183(2):146-150. doi:10.1016/s0002-9610(01)00863-7
- Santosa KB, Priest CR, Oliver JD, et al. Influence of faculty diversity on resident diversity across surgical subspecialties. The American Journal of Surgery. 2022;224(1, Part B):273-281. doi:10.1016/j.amjsurg.2022.02.009
- Keane AM, Larson EL, Santosa KB, et al. Women in Leadership and Their Influence on the Gender Diversity of Academic Plastic Surgery Programs. Plast Reconstr Surg. 2021;147(3):516-526. doi:10.1097/PRS.0000000000007681
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 16 October 2024
TITLE: Data Studio Office Hour
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
ZOOM MEETING INFORMATION:
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
—
DATE: Wednesday, 9 October 2024
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio
TITLE: Co-design a Fisheries Model for Nature Base Solutions
INVESTIGATORS:
Julian Olaya (1,2)
Jade Delevaux (1)
Gretchen Daily (1,2,3)
(1) Woods Research Natural Capital Project
(2) Biology
(3) Stanford Woods Institute for the Environment
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Coral reefs and mangroves are ecosystems that provide essential ecosystem services upon which millions of people depend (fisheries, food, employment, recreation, coastal erosion protection, etc.). However, they are severely threatened by global warming and the loss of natural cover due to human activities. One strategy to prevent the loss of these ecosystems and their benefits is nature-based solutions, such as active restoration, where mangrove trees and coral colonies are actively planted in degraded areas, increasing natural cover and ecosystem complexity. We aim to evaluate how this restoration affects the distribution and abundance of target fishery species.
HYPOTHESIS & AIM
Understanding and quantifying the benefits of restoration will allow the expansion of these activities to many places around the world. We hypothesize that increased coral cover and three-dimensional complexity of these ecosystems will increase the abundance of fish dependent on them, which in turn will increase the abundance of their predators, species of high commercial value in fisheries. The main objective of this study is to predict how the distribution and abundance of target fishery species increases as the cover and complexity of ecosystems are restored.
DATASET
This study uses data collected throughout the National Coral Reef Monitoring Program (NCRMP), that evaluate benthic community structure and fish community. The NCRMP provides a biennial ecological characterization at a broad spatial scale of general reef condition for reef fishes, corals and benthic habitat. The goal of the coral demographic surveys is to collect information on species composition, density, size, abundance, and specific parameters of condition (% live vs. dead, bleaching, disease) of non-juvenile scleractinian corals (>4 cm maximum diameter), and of overall species diversity (all corals) using 10m-by-1m belt transects in a stratified random sampling design in hardbottom and coral reef habitats.
The fish community surveys collect information on species composition, density, size, abundance, and derived metrics (e.g., species richness, diversity) using the RVC method in a stratified random sampling design on hardbottom and coral reef habitats. The RVC method occurs with the diver remaining at a fixed site. Fish are surveyed within an imaginary 15-m diameter cylinder centered on the diver and extending vertically from the substrate to the limits of vertical visibility.
STATISTICAL MODELS
Our goal is to develop a model to predict how fish abundance responds to changes in ecosystem characteristics. We will explore the relationships between ecosystem variables and fish abundance to understand which factors most influence fish populations. Ultimately, we aim to predict how increasing coral cover or mangrove area can benefit fisheries (high abundance of target species).
STATISTICAL QUESTIONS
(1) What is the distribution of fish abundance and ecosystem variables?
(2) What is the relationship between fish abundance and specific ecosystem variables (e.g., coral cover, mangrove area)?
(3) Which model (e.g., linear, generalized linear, or non-linear, or other) can be built to predict fish abundance based on these variables?
(4) How sensitive are the predictions to changes in the input variables?
(5) Can time series models be used to capture temporal trends and seasonality in fish abundance and ecosystem variables?
(6) Can we identify a relationship between fish species, such that when species X is abundant, species Y is also abundant?
(7) Is there a significant correlation between the abundance of fish species, controlling for environmental variables?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 2 October 2024
TIME: 3:00–4:30 PM
TITLE: Investigating Conformational Templating in the Human Proteome
INVESTIGATORS:
Isabel Larus (1)
Dan Jarosz (1, 2)
(1) Department of Chemical and Systems Biology
(2) Department of Developmental Biology
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
The recent discovery that proteins can function in non-stoichiometric assemblies called biomolecular condensates has sparked a revolution in cell biology. Condensates often form through liquid-liquid phase separation, but can adopt diverse material states and impact a wide variety of biological activities. The handful of examples studied in detail have led to a prevailing assumption that most condensates exist transiently. However, some others can self-template, generating stable changes in function that can transmit and amplify biological information through structural replication. An extreme form of this behavior can be seen in toxic conformers formed by the mammalian prion protein (PrP) and some other proteins linked to neurodegeneration. Moreover, some disease-associated variants in such proteins strongly impact structural replication. At the same time, structural replication is critical for many proteins’ normal functions in processes ranging from innate immunity to long-term memory. There are currently no proteome-wide measurements of self-assembly and -templating capacity in humans or any other organism. Thus, we have a fragmentary understanding of the prevalence and potential physiological roles of self-templating and its biochemical and biophysical underpinnings and how these properties are affected by genetic variation.
HYPOTHESIS AND AIM
This project aims to create a quantitative atlas of self-assembly and self-templating in the human proteome to understand how variation in protein sequence and levels impact these properties. Our lab has developed a degron-based assay that couples protein stability to a DNA sequencing output, enabling quantitative and scalable measurements of protein self-assembly and self-templating for nearly any protein. We used this method to examine the human ORFeome (~15,000 cloned proteins), employing the model organism S. cerevisiae as a living test tube. This approach identified known condensates and self-templating proteins as well as other proteins with these properties with novel sequence features. We hypothesize that the data will also enable us to quantify differences in assembly state, duration of replication, and toxicity.
DATASET
Our reporter capitalizes on a universal feature of protein assembly – enhanced stability – by employing a destabilizing domain (DD). Monitoring the stability of fusions to these degrons permits in vivo limited proteolysis experiments with single-cell resolution. Our reporter fuses query genes to an N-terminal selectable marker and a C-terminal DD tag. Most proteins are rapidly degraded. However, those that form aggregates and condensates are more resistant to proteolysis. Because degradation is directional, protein assembly also shields the N-terminal selectable marker, allowing us to identify ‘winners’ and ‘losers’ by serial competition and deep sequencing. Under ideal conditions this assay produces a six order of magnitude difference in signal between natively folded and self-templating protein conformers and shows a limit of detection as low as 1 kcal/mol for differences in stability. Our 46-sample dataset consists of longitudinal next generation sequencing read counts for each human query ORF (five timepoints) in triplicate serial competitions under conditions that probe the relationships between expression, stability, and fitness.
STATISTICAL MODELS
First, we would like to build a model that describes self-assembly and self-templating capacity across the proteome, incorporating information from all three of our experimental conditions and five time points. Second, we want to leverage this dataset to perform both unbiased and targeted analyses of how amino acid sequence and biophysical features shape these behaviors. We plan to use this tool in future studies, specifically to measure the effects of chemical or genetic perturbations, cross-seeding, stress, and aging. We would welcome feedback on experimental design and statistical approaches to maximize the power of those experiments.
STATISTICAL QUESTIONS
- What is the best statistical method to describe and quantify the longitudinal behavior of a given protein in our assay, incorporating data from the three different conditions and five time points which would best enable comparisons of stability and self-templating between different ORFs.
- What statistical methods can be leveraged to quantify the toxicity associated with over-expressing an ORF and/or it’s capacity to adopt a toxic self-templating state?
- How can we leverage this dataset to identify sequence and biophysical features that may drive self-templating?
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
DATE: Wednesday, 25 September 2024
TITLE: Data Studio Kickoff Meeting
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
AGENDA
The first session of Data Studio for the Autumn Quarter, also available as BMDS 291 for students, will include faculty-student introductions, a review of the course syllabus, and an introductory lecture about the art of data science consultation. If you wish to learn more, you are welcome to attend either in-person or via Zoom videoconference.
ZOOM MEETING INFORMATION
Join from PC, Mac, Linux, iOS or Android:
https://stanford.zoom.us/j/93494617954?pwd=28xCchr71hDZ1136Ny6cwGX9rvOhJs.1
Meeting ID: 934 9461 7954
Password: 158353
Or iPhone one-tap (US Toll):
Or Telephone:
Dial: +1 650 724 9799 (US, Canada, Caribbean Toll) or
+1 833 302 1536 (US, Canada, Caribbean Toll Free)
Meeting ID: 934 9461 7954
Password: 158353
Meeting ID: 934 9461 7954
Password: 158353
Spring Term 2024
DATE: Wednesday, 5 June 2024
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
DATE: Wednesday, 29 May 2024
TITLE: Association of Individual Surgeon Volume with Postoperative Outcomes in Heart Transplantation
INVESTIGATORS:
Vikram Fielding-Singh (1)
Bharathram Vasudevan (1)
Matthew William Vanneman (1)
Louise Sun (1)
(1) Anesthesiology, Perioperative and Pain Medicine (Cardiac)
ABSTRACT:
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
Introduction
Heart transplant is the definitive therapy for patients with end-stage heart failure. Prior work has shown an association between center volume and survival after heart transplantation. However, the association of individual surgeon-specific volume with heart transplant outcomes remains unknown.
Hypothesis
We hypothesized that lower surgeon and center volume are associated with postoperative mortality after heart transplantation.
Data
We identified all adult (18 years) patients who underwent orthotopic heart transplants in the US from 2011 to 2022 in the United Network for Organ Sharing (UNOS) Standard Transplant Analysis and Research data file. Patients undergoing multi-organ transplants were excluded.
Variables
Surgeon and center volume for a specific patient at the time of the surgery were defined as the rolling number of transplants in the 365 days prior to transplant date. Surgeons and centers were stratified into low (0-9/year), medium (10-29/year), and high volume ( 30/year). The primary outcome was 1-year postoperative mortality. Secondary outcomes were postoperative stroke, postoperative dialysis, and treatment for rejection within 1 year of transplant.
Statistical Models
We fitted a multilevel Weibull proportional hazards model for the primary outcome and multi-level logistic regression for secondary outcomes, with surgeon-level random effects nested within center-level random effects. All analyses were performed using Stata version 18.1 (StataCorp LP, College Station, TX, USA). A p value < .05 was considered significant.
STATISTICAL ISSUES
1) We are interested in whether our modeling approach is correct.
- a) How do we tease out the best way to model surgeon volume, center volume, as well as surgeon and center unobserved characteristics?
- b) Specifically we are interested in whether the use of nested surgeon- and center-level random effects (while also having surgeon or center volume as variables in the model) is the correct way to approach this question.
- c) This may involve understanding how Stata models mixed effects – a link to the Stata documentation that describes the Methods and formulas for the command we are currently using is here: https://www.stata.com/manuals/me.pdf#memestreg
2) I am also interested in whether the methods from this paper can be applied to this project – doi:10.1001/jama.2019.15686. Is survival benefit a concept that could be applied here?
3) I am also very interested in whether the way that a transplant program organizes its surgical call volume is related to survival benefit. For example, some programs have many surgeons taking a small amount of call and doing a small number of transplants. Others have a small number of surgeons on call who then do a lot of surgeries. We can look at how centers are organized because we have surgeon and center IDs, but I’m not sure exactly how to describe the different patterns in a systematic way.
DATE: Wednesday, 22 May 2024
TITLE: Evaluation of neuropsychiatric changes after vaccine administration and fever episodes in Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS)
INVESTIGATORS:
Jaynelle Gao (1)
Janell Sherr (1)
Jennifer Frankovich (1)
- Department of Pediatrics
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
PANS is defined by the abrupt onset of severe neuropsychiatric symptoms. Relapses occur in the setting of immune activation (infections, febrile illnesses, etc) raising concern around vaccinations. We hypothesized that flares would be more pronounced following febrile illnesses compared to vaccines.
AIMS & HYPOTHESIS
The primary aim of this study is to compare neuropsychiatric deteriorations (flares) associated with febrile illness to those associated with routine childhood vaccination in a community cohort of patients with PANS. We hypothesize that (1) the frequency of flares associated with febrile illnesses is higher than that of flares associated with vaccinations; (2) flares associated with febrile illnesses last longer than do flares associated with vaccinations; and (3) flares associated with febrile illnesses are more severe (i.e., treated less aggressively) than those associated with vaccines.
DATASET
Our study included patients based on pre-defined criteria (meet PANS criteria…). For our study cohort, we collected dates of all documented vaccine administrations and febrile illnesses that occurred after the patient’s first clinic visit. Chart review included all patients seen between _ and August 1, 2021. For each event (vaccine or febrile illness), an associated flare was defined by clinician documentation or parent report of new or worsening neuropsychiatric symptoms within one month or three clinic visits of vaccine administration or febrile illness onset. For each flare, we also collected start/end dates and treatment modality.
STATISTICAL MODELS
We are planning to use descriptive statistics to demonstrate the frequency and duration of flares associated with vaccination.
STATISTICAL QUESTIONS
- What is the best way to handle this paired data? Some patients have never had a documented vaccine or a febrile illness, some have had both, and others have only had one or the other.
- For patients who have more than one flare associated with febrile illness or more than one flare associated with vaccine, would it be appropriate to average the events so that each patient is only counted once?
- Do we have enough power to subcategorize the vaccine events into vaccines given at good baseline vs. high-risk vaccines (e.g, vaccines given during an illness, during an existing flare, or during reduction of anti-inflammatory therapy)?
DATE: Wednesday, 8 May 2024
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project. This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/). Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday. If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians.
DATE: Wednesday, 1 May 2024
TITLE: Optimizing Medicaid Managed Care to Improve Access, Quality, and Clinical Outcomes for Patients with Gastrointestinal Cancers
INVESTIGATOR:
Aaron J. Dawes, MD, PhD (1,2)
(1) Section of Colon & Rectal Surgery, Department of Surgery
(2) Stanford-Surgery Policy Improvement Research and Education Center (S-SPIRE)
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Millions of Medicaid enrollees with cancer have been transitioned from fee-for-service (FFS) to comprehensive managed care plans over the past decade with unknown effects on access, quality, and clinical outcome. Patients with gastrointestinal (GI) cancers require timely and coordinated access to multiple specialty providers (e.g., medical oncologists, radiation oncologists, and surgeons) to avoid progression of their disease. Patients who are unable to navigate potential barriers to receiving care—especially patients with higher levels of social vulnerability—may experience delayed, substandard, or even forgone care and worse cancer outcomes. There is, therefore, a critical needto determine how patients with GI cancers were impacted by the transition to Medicaid managed care (MMC) in order to address any potential gaps in care before they affect clinical outcomes.
HYPOTHESIS & AIMS
Aim 1: Quantify changes in access to care, quality of care, and clinical outcome that occurred as a result of the transition to MMC. I will use causal inference modeling to compare measures of access and quality of cancer care as well as 5-year survival between patients living in transitioning and non-transitioning counties before and after the transition to MMC (a “difference-in-differences” approach). Hypothesis: Patients travelled further and waited longer to see a surgeon, were less likely to receive guideline-concordant care, and were more likely to die following their diagnosis as a result of the transition to MMC.
Aim 2: Compare differences in access, quality, and clinical outcome that occurred as a result of the transition to MMC by cancer type and level of socioeconomic disadvantage. I will compare the impact of MMC between patients based on cancer type and neighborhood socioeconomic disadvantage (a heterogenous treatment effects model). Hypotheses: 1) Patients who require coordinated services (e.g., chemotherapy, radiation, and surgery) and 2) patients from areas with more socioeconomic disadvantage will experience larger differences in access, quality, and clinical outcome.
Aim 3: Evaluate changes in provider networks that occurred as a result of the transition to MMC. I will construct a model of each county’s cancer care provider network using Medicaid claims data. I will then utilize my difference-in-differences framework to isolate the causal effects of the transition to MMC on county-level measures of network composition. Hypothesis: Specialty cancer networks will have a lower provider-to-enrollee ratio and a lower percentage of available providers included in network as a result of the transition to MMC.
DATASET & SAMPLE
Data for all three aims will be drawn from the linkage of three files: 1) patient-level data from the California Cancer Registry (CCR), 2) patient-level Medicaid claims and enrollment files, and 3) county-level data from the California Department of Health and Human Services (CalHHS). CCR is the largest statewide cancer surveillance system in the United States and contains longitudinal data on treatment and clinical outcomes for all patients diagnosed with cancer in the state. I currently have data on all GI cancers diagnosed in California between 2010-2020 (approximately 811,000 patients). The CMS Chronic Conditions Warehouse has already linked these data to administrative records from a 100% Medicaid file owned by Stanford University and provided the appropriate data crosswalks. To our knowledge, this linked CCR-Medicaid file is unique and represents a powerful tool for understanding both utilization and clinical outcomes.CalHHS publishes county-level data on Medicaid enrollment on a monthly basis, including the number and percentage of enrollees in FFS vs. MMC. I will use these data to classify counties as switching vs. non-switching based on the date of their transition to MMC. Patients will be categorized based on their county of residence at the time of diagnosis.
Because Medicaid enrollment can change on a monthly basis, I will begin with patients who were continuously enrolled for the 6 months prior to their diagnosis, but plan to explore patients with discontinuous enrollment patterns (“churn”) in sensitivity analyses. I will also stratify patients based on their reason for Medicaid eligibility (as denoted by their Medicaid aid code) for two reasons. First, since Medicaid expansion and MMC transition occurred at similar times, certain patients may not have been eligible throughout the study period. I will begin by looking at all Medicaid patients regardless of their aid code, but plan to limit my analyses to patients who would have been eligible for the entire time period as a sensitivity analysis in order to isolate the transition effect from the expansion effect. Second, as noted above, different aid codes transitioned to mandatory MMC at different times in certain switching counties. Stratifying by aid code is therefore necessary to correctly classify patients. Patients with both Medicaid and Medicare coverage (“dual eligibles”) will be excluded from all analyses since they are not required to enroll in MMC in California.
STATISTICAL MODELS
I will utilize a difference-in-differences (DD) framework. In California, 14 counties mandated MMC enrollment prior to Medicaid expansion (non-switching counties; control). On expansion, all but one of the remaining counties transitioned their FFS patients into MMC (switching counties; treatment). 27 switching counties made a sharp transition from FFS to MMC; the remaining 16 switching counties made a more gradual change. I have started with the sharp transitions for simplicity, but would like to extend my analyses to the gradual counties to improve power and generalizability.
To test the parallel trends assumption, I will plot quarterly rates of each outcome during the post-transition period because I am using an always-treated instead of a never-treated control group (“reverse DD”). I will then estimate a Two-Way Fixed Effects (TWFE) DD regression model for each outcome after adjusting for individual-level covariates (age, sex, tumor site, tumor histology, stage at diagnosis, and Charlson Comorbidity Index), year of diagnosis, intervention group (switching vs non-switching county), time period (pre- vs post-transition), and an interaction term between intervention and time period, which represents the adjusted DD estimator. Correlations within geographic units will be accounted for by heteroscedasticity-robust standard errors clustered at the county level. A significant coefficient on the adjusted DD estimator will be interpreted as evidence of a causal effect of MMC on that outcome measure.
STATISTICAL QUESTIONS
- How should I test the assumptions of my DD model? How do these change with a reverse DD? What additional analyses would you expect to see for a DD design like this?
- What do I do if I do not have parallel trends in the post period? How can I adjust my model?
- What are the major threats to causal interpretation? Do my current sensitivity analyses sufficiently separate expansion effects from transition effects? What additional sensitivity analyses should I plan to perform to investigate causality?
- How can I best utilize data from counties with a graduation transition from FFS to MMC?
DATE: Wednesday, 24 April 2024
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. For assistance with bioinformatics analysis and pipeline development, please contact the Bioinformatics as a Service team (mailto:gbsc-baas-team@lists.stanford.edu) for a free consultation. If you need to purchase bioinformatics software, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/).
DATE: Wednesday, 17 April 2024
TITLE: Antimicrobial therapy of Enterococcal bacteremia: a retrospective comparison of outcomes with IV or oral antimicrobial therapy
INVESTIGATORS:
Caitlin A. Contag (1)
Hector F. Bonilla (1)
- Division of Infectious Diseases, Department of Medicine
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Enterococci are one of the most common causes of hospital-associated infections. They are associated with endocarditis, intra-abdominal infections, urinary tract infections, catheter-associated infections, and other infections that lead to significant morbidity and mortality. The best outcomes are observed in patients who receive a combination of antibiotic therapy. There are limited data demonstrating that switching to oral therapy is equal to the current standard of care.
OBJECTIVE
Analysis of Enterococcus bacteremia in adults epidemiological, clinical, microbiological, and prognostic characteristics.
STUDY DESIGN
This is a retrospective study of adults from a single tertiary medical center in patients hospitalized with Enterococcal bacteremia. We excluded polymicrobial bacteremia and patients who died during index hospitalization.
DATA
The bacteremia cases were identified using the Stanford microbiology database, STARS, and clinical data was obtained using the Stanford Health Care EPIC system. We identified 473 cases of enterococcus bacteremia (E. faecalis 256; E. faecium 182; E. Avium 14; E. Casseliflavus 10; E. Gallinarum 8; E. Raffinous 2 and E. Species 1). These are the therapeutic regimens that were administered:
1) Intravenous antimicrobial therapy only (e.g., Ampicillin, ampicillin/ceftriaxone, ampicillin/gentamicin, vancomycin, daptomycin, linezolid)
2) Intravenous therapy transitioned to oral therapy (e.g., amoxicillin, ampicillin, linezolid)
3) Oral antimicrobial therapy only
OUTCOME MEASURES
From the data, we obtained the following outcomes of interest: Length of stay (median, IQR), Recurrent bacteremia within 30 days, and Mortality (30, 60, 90 days).
STATISTICAL QUESTIONS
- Is there a significant difference in mortality, bacteremia recurrence, or readmission risk when comparing patients who received only IV antibiotics to those who received some or all oral therapy?
- Is oral treatment safe and effective in treating Enterococcal bacteremia?
DATE: Wednesday, 10 April 2024
TITLE: CRISPR-engineered Protein Barcodes Matched with Single-Cell Specific Interference Enables High-Content Screening for Targetable Histone Modifiers in Glioblastoma
INVESTIGATORS:
Dena Panovska (1)
Janne Van Hauwenhuyse (2)
Dirk Daelemans (2)
Frederik De Smet (2)
- Stanford University
- KU Leuven, Translational Cell and Tissue Research
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Isocitrate dehydrogenase (IDH) wild-type high-grade glioma (i.e., glioblastoma, GBM) is an aggressive primary brain cancer associated with poor response to standard-of-care (SoC) therapy whereby disease recurrence is driven by immense cellular heterogeneity. High-content, pooled single-cell CRISPR (scCRISPR) screens provide an unprecedented way for discovering novel targets in heterogeneous and complex diseases.
HYPOTHESIS & AIM
The role and action of histone-modifying enzymes in GBM is not well understood. Moreover, targeting histone modifiers may lead to decreased cell proliferation and apoptosis, thus paving the way to develop targeted therapies for patients with GBM. The purpose of this study is to discover novel therapeutic targets through inhibition of histone-modifying enzymes while considering GBM’s heterogeneity and cellular plasticity. In summary, there are three main research questions:
- Does histone enzyme knockout cause decrease in cell proliferation?
- Does histone enzyme knockout cause phenotypic changes (cellular plasticity)?
- Given the heterogeneity, is there a difference in the effects of the gene knock-out between two cell line models and unmodified controls?
EXPERIMENTAL PROCEDURE
Here, we designed triplets of 13 artificial protein sequences which resulted in 286 (i.e., 13 choose 3) unique barcode combinations. Each barcode was associated with a gRNA targeting a single gene-encoding histone-modifying enzyme. As such, we generated two libraries containing four gRNAs per gene targeting approximately 100 genes in total. The plasmid libraries were transduced in two patient-derived cell lines generated from a single patient. The first cell line represents the treatment naïve tumor (CME037) and the second one, progressing disease (CME038).
As a readout, a CyTOF antibody panel was tailored, which measured the barcode combinations, GBM cellular subtype, histone modification, and cell proliferation capacity. Cells were harvested and measured at three timepoints in three biological and technical replicates, along appropriate control samples.
EXPERIMENTAL DESIGN
So far, data was collected from timepoint 1 (approximately 15 million cells) and 2 (around 80 million cells), distributed among 3 biological and 3 technical replicates. Each sample contains around 2 million cells. Within each sample, cells are distributed among 286 barcode populations.
The single-cell protein marker measuring panel distinguishes cell populations based on surface barcodes (combination of 3 out of 13 markers = 286) and biological markers (n = 24, proliferation, cell phenotype, histone markers).
STATISTICAL QUESTIONS
The main problem that we have with this dataset is the large number of cells per population, and whenever we make comparisons, we always end up with significant p values.
- Which correction method should be applied on the registered p-values?
- Which statistical test is the best to use to show statistical changes in cellular proliferation between knock-outs and wild-type cells?
- Which statistical test will show us the significant change in cell phenotype?
- How should we integrate everything and compare changes between cell lines longitudinally? What statistical model or test should we use?
DATE: Wednesday, 3 April 2024
AGENDA: This will be the first session for the Spring Quarter.
The agenda is:
1. Introductions: Faculty and Students
2. Dr. Tamaresis will review the syllabus with the students and present a lecture about the art of statistical consultation.
Winter 2024 term
DATE: Wednesday, 13 March 2024
TITLE: A Phase 2 Study of Magrolimab and Pembrolizumab in Relapsed or Refractory Classic Hodgkin Lymphoma
INVESTIGATORS:
Ranjana Advani (1)
Joseph Schroers-Martin (1)
- Stanford Cancer Institute
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
Background
The Stanford clinical trial LYMHD0019 is a single-arm phase II investigator-initiated trial of the combination of magrolimab and pembrolizumab in relapsed/refractory classic Hodgkin lymphoma (R/R cHL), planned to enroll up to n=24 patients.
· Pembrolizumab is a checkpoint inhibitor immunotherapy (CPI) which is FDA-approved for the treatment of relapsed/refractory Hodgkin lymphoma and has been assessed both as monotherapy and in chemotherapy combinations.
· Magrolimab is an investigational immunotherapy agent targeting the CD47 protein, an immune checkpoint overexpressed in many cancers and specifically overexpressed in Hodgkin Reed-Sternberg cells.
· The clinical trial protocol was initially approved 6/26/2020 as a single arm, phase II study. To date 8 patients have been enrolled at two sites (Stanford and Dana Farber Cancer Institute).
Magrolimab is under investigation in other cancers including leukemias and solid tumors. Recently, the FDA placed the drug under full clinical hold in leukemias based on the results of the three studies in myeloid blood cancers (ENHANCE1-3).
· In each of these studies, there was a higher risk of death in the group of patients who received magrolimab compared to the group of patients who received standard treatment.
· In both the ENHANCE and ENHANCE-3 studies, there was a higher risk of serious side effects that resulted in death, particularly from infections as blood infections and lung infections.
Based on these findings, the Stanford trial is currently on partial clinical hold (continued treatment for existing patients, no new enrollments) pending a response to several FDA requests:
· “Revise the study to include a control arm in order to allow for meaningful interpretation of safety results in the magrolimab combination cohorts and provide justification for the chosen control arm.”
· “Considering the results of […the leukemia studies…], comment on the benefit-risk profile of continued evaluation of magrolimab in patients with relapsed and refractory cHL. Provide data-based justification for the continued study of each magrolimab dose and combination that is intended for further evaluation”
Statistical considerations
We would like assistance with providing a statistically meaningful response to these FDA requests, including:
1. Interpretation of safety of the combination regimen
2. Justification for continued study of the current dose regimen.
There are several difficulties with the request to add an interventional control arm in the trial:
· The logical control arm for the magrolimab/pembrolizumab combination would be single agent pembrolizumab. Pembrolizumab is FDA-approved for R/R cHL, so most patients will have already received this either alone or in a chemotherapy combination. It would not be clinically appropriate to re-treat with a prior therapy after disease progression.
· Even with a matched control arm, with a planned enrollment of n=24 patients it seems unlikely that we would have power to “allow for meaningful interpretation of safety results in the magrolimab combination cohorts”.
· There is extensive historical data regarding the safety of pembrolizumab monotherapy in R/R cHL, including the landmark KEYNOTE-087 trial (n=210).
In the initial statistical design of the trial, the primary efficacy endpoint is the CR rate and key secondary endpoints include ORR, DOR, PFS, OS.
· As a single arm phase 2 study, the control group is historical subjects receiving a single-agent PD1 inhibitor (including PD1-inhibitor-naïve patients and patients who previously received a PD1 inhibitor). For historical subjects with R/R cHL PD-1 inhibitors have a CR rate of approximately 18%.
· With the combination of magrolimab and pembrolizumab, we hypothesize that the CR rate will be approximately 40%. Setting a null hypothesis of 18% and an alternative hypothesis of 40%, a sample size of 24 subjects would provide 80% power with a 1-sided alpha error rate of 0.01.
Data Sets
· Retrospective historical data:
o KEYNOTE-087 trial of pembrolizumab monotherapy (n=210)
· Prospective data:
o n=8 patients enrolled to date
Statistical questions
1. How would we best leverage historical data to provide a statistically meaningful control for patient safety with pembrolizumab monotherapy?
2. Can we justify safety of the current dose regimen based on the patient experience to date and historical control date?
3. Can we demonstrate that meaningful safety data cannot be achieved via an interventional control arm given the anticipated enrollment?
DATE: Wednesday, 6 March 2024
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
DATE: Wednesday, 28 February 2024
TITLES:
- A) Nonlinear Mixed Effects model for a 3-parameter Logistic Curve
- B) Prediction of Gene Expression on Histopathology Images
INVESTIGATORS:
- A) Aditi Goyal (1)
- B) Susie Avagyan (1)
(1) Biomedical Data Science
ABSTRACTS
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, we have a Data Studio Double-Header Workshop. We have two investigators each of whom will discuss a project with the group.
- A) ADITI GOYAL
I’m trying to create a non-linear mixed effects model for a 3-parameter logistic curve. I’m working with an immunology group that is aiming to determine parallelism in their bioassays, and they’ve given me a method to duplicate. I have some documents, and I’m currently trying to implement the math in R.
- B) SUSIE AVAGYAN
INTRODUCTION The need to develop computational methods to examine spatial transcriptomics data has become increasingly urgent with the rapid progress in spatial sequencing technologies. It is essential to analyze this data to characterize cell communities and identify spatial biomarkers for diseases, shedding light on how different cells within a tissue organize themselves to support tissue functions and drive biological processes. However, grappling with the volume and complexity of spatial transcriptomics data and its associated data modalities poses a significant challenge in conducting thorough analyses and making meaningful inferences about the spatial localization of disease biomarkers.
HYPOTHESIS & AIM We focus on graph-based autoencoders and utilize them for the integration of gene expression, cell adjacency (based on spatial coordinates), and histology images. The goal of using this model is to construct a robust joint latent space of the integrated data modalities, which can be used for several downstream applications. From the downstream applications, we are considering gene expression prediction given only a histology image of a tumor specimen and identification of spatially localized cellular communities and gene expression patterns.
DATASET The datasets for training and test sets will be accessed from MERSCOPE FFPE Human Immuno-Oncology Data Release This data comprises 16 patient samples from different cancer types, from which 14 will be used for training and cross-validation, and 2 patients will be held to assess the final performance of the model. The modalities available in the datasets are spatial organization of single cells (8,696,580 cells, ~500K per sample), gene expression for each cell (500 gene panel), and histology images of the sequenced tissue.
STATISTICAL ISSUES
- A) ADITI GOYAL I’m a little stuck on how to implement the NLME in R.
- B) SUSIE AVAGYAN
1) Choice of statistical model for gene expression: Due to the sparsity in scRNA-seq data, instead of exact reconstruction, models have been explored that only estimate the parameters of a statistical model of gene expression. For example, model gene expression by predicting the parameters of a zero-inflated negative binomial (ZINB) distribution. However having only a gene panel of 500 genes, there isn’t as much sparsity in our data.
- What models can we explore to model gene expression in this case?
- Is this number of features too few to construct a robust latent space, also given the use of other data modalities?
2) Choice of statistical methods for evaluation of the performance: For the downstream task of predicting gene expression, we think to compute the Pearson’s and Spearman’s correlations between the expression predicted by our model and ground truth. However, we also want to measure the “spatial accuracy” of predictions, meaning how accurately the model predicts spatial regions where the gene expression is high or low.
- What metrics can we use to assess this?
- What else would you recommend for assessing the performance of this task?
DATE: Wednesday, 21 February 2024
TITLE: Antisense oligonucleotide therapeutic approach for Timothy syndrome
INVESTIGATOR:
Xiaoyu Chen (1)
- Psychiatry and Behavioral Sciences
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Timothy syndrome (TS) is a severe multi-system disorder characterized by autism, epilepsy, long QT syndrome and other neuropsychiatric conditions1. TS type 1 (TS1) is caused by a gain-of-function variant in the alternately spliced and developmentally enriched CACNA1C exon 8A, as opposed to its counterpart exon 8. We previously uncovered several phenotypes in TS1 patient-derived neurons, including delayed channel inactivation, prolonged depolarization-induced calcium rise, impaired interneuron migration, activity-dependent dendrite retraction and an unanticipated persistent expression of exon 8A. We reasoned that switching CACNA1C exon utilization from 8A to 8 represents a possible therapeutic strategy. Here, we developed antisense oligonucleotides (ASO) to effectively decrease exon 8A inclusion in human cells both in vitro and, following transplantation, in rodents. We discovered that the ASO-mediated exon 8A to 8 switch robustly rescued defects in patient-derived cortical organoids and migration in forebrain assembloids. Leveraging a transplantation platform we developed, we found that a single intrathecal ASO administration rescued calcium changes and in vivo dendrite retraction of patient neurons, suggesting that suppressing CACNA1C exon 8A expression is a potential treatment for TS1. Broadly, these experiments illustrate how a multi-level, in vivo and in vitro stem cell model-based approach can identify strategies to reverse disease-relevant neural pathophysiology.
HYPOTHESIS & AIM
Previous studies have shown a splicing defect of CACNA1C in neurons derived from Timothy syndrome induced pluripotent stem cells (hiPSC). We hypothesized that correcting this splicing defect by ASO can potentially reverse disease phenotype. We performed in vitro drug discovery (from brain organoids of TS hiPSC) in vitro, then validated their rescuing effects in vivo on brain organoids that were transplanted into rat cortex.
DATASET
We have previously obtained three individuals that were diagnosed with TS, and generate hiPSCs from their fibroblast. Using this three individual cell lines, together with three cell lines derived from healthy individuals, we have performed the following assays and dataset.
- Collecting RNA samples from the brain organoids derived from the above mentioned cell lines (3 Control and 3 TS). These cell lines are differentiated into brain organoids for multiple times. Brain organoids were collected from several batches of experiments at different time of the differentiation and by different researchers (day 30, day 60 and d90). These samples were then measured for the levels of different isoforms of CACNA1C. We used ANOVA, then compared TS vs. ctrl at day 30, day 60 and day 90.

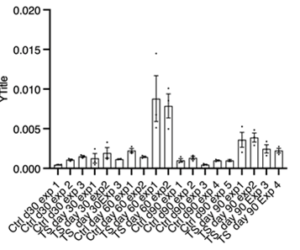 Dataset structure (for left panel)
Dataset structure (for left panel)
- We then designed an array of small molecules that can potentially interfere the abnormal splicing of TS CACNA1C. In total 22 molecules were applied to the organoids (derived from three TS patients). We than probed the pharmacokinetics and pharmacodynamics of several promising molecules on the brain organoids.
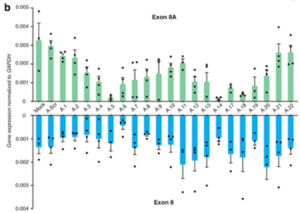
The 4 data points are from 2 TS lines, each line received 22 separate molecule in duplicates. Large amount of organoids from each of the two TS line were dissociated into cell culture coverslips. Each ASO (small molecule) was applied to two coverslips of the each TS neuronal culture, generating 2*2=4 data points. We didn’t perform any statistical comparison.
- We chose one promising molecule for in vivo validation. Hit molecule was injected intrathecally into rat brain. These rats were immunocompromised and transplanted with the above mentioned human brain organoids. Those organoids mature overtime. After 10-14 days, rat cortex, rat cerebellum, human organoid grafts were collected and processed for isoform measurement.
On left, each point represents an animal. On right, each point represents a single organoid that grafted in rat brain.
STATISTICAL QUESTIONS
(1) Should we use ANOVA or t-test if our question is whether there’s any difference between control and TS?
(2) Can we still perform comparison of data set no. 2?
(3) Dataset no. 3, similar question as (1), should we use ANOVA or t-test if our question if whether there’s any difference between PBS (vehicle) vs. ASO (treatment) groups?
(4) In stem cell research, researchers only reprogram pluripotent stem cells once and we treat each differentiation as biological replicate instead of technical replicate. More and more people are using organoids as their disease model to do research, what count as biological replicate? Some use a single organoid as a biological replicate, some view a single organoid as a technical replicate, how would this affect analysis?
DATE: Wednesday, 14 February 2024
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
DATE: Wednesday, 7 February 2024
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
DATE: Wednesday, 31 January 2024
tps://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
DATE: Wednesday, 24 January 2024
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
DATE: Wednesday, 17 January 2024
TITLE: Trajectories and Predictors of Loneliness during the First Year of COVID-19: A Longitudinal Study (COVID-19 WELL)
INVESTIGATORS:
Xiaoyan Zhang (1)
Ann Hsing (1)
Ying Lu (2)
(1) Stanford Prevention Research Center
(2) Biomedical Data Science
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Loneliness is a public health concern with a high prevalence and has harmful health and economic impact. Findings on the changes of loneliness during the pandemic are mixed, suggesting there might be inter-individual differences in loneliness as the pandemic progressed. The heterogeneous nature of loneliness was evident, characterizing by a substantial variability in the severity (low, medium, or high) and stability (stable, increasing, decreasing) of the patterns during the early phase of the pandemic. However, gaps remain in understanding how loneliness has persisted or re-emerged throughout the first year of the pandemic and the risk and protective factors associated with these trajectories.
HYPOTHESIS & AIM
This study aims to identify trajectory patterns of loneliness during the first year of the COVID-19 pandemic and to investigate their relationships with selected sociodemographic and psychosocial factors including race, gender, employment status, history of depression diagnosis, meaning and purpose, perceived social support and psychological resilience. We hypothesize that:
- There are at least 3 trajectories: stable low, medium, and high.
- the stable low trajectory would be characterized by consistently low loneliness (below average loneliness score) across all 5-time points.
- the stable medium trajectory would be characterized by consistently medium loneliness across all 5-time points.
- the stable high trajectory would be characterized by consistently high loneliness across all 5-time points.
- Using the Stable Low Trajectory as the reference group, baseline meaning and purpose, perceived social support and psychological resilience are significant predictors of the Stable High Loneliness Trajectory (lower odds of being in the Stable High Loneliness Trajectory compared to being in the Stable Low Trajectory) while risk factors such as being female and unemployed, and history of depression diagnosis predict the membership of higher loneliness class (higher odds being in the Stable High Loneliness Trajectory).
DATASET
This study uses data from the COVID-19 and Well-Being Study (COVID-19 WELL), a sub-study within the Stanford WELL for Life Study (WELL Study). The COVID-19 WELL is a 1-year study with repeated measurements at six time points to evaluate the short- and long-term impact of loneliness related to COVID-19 over time. The study collect data at six time points: Baseline (T0, March 23-April 2), Day 10 (T1, April 2-April 17), Month 1 (T2, April 23-May 2), 3 (T3, June 23), 6 (T4, September 23), and 12 (T5, March 23, 2021). We exclude T4 data in our study due to lack of loneliness data. We plan to use the sociodemographic and psychosocial factors from the baseline (T0) to predict emerged trajectories; however, they are available in all five time points. The analytic sample size is 927.
STATISTICAL MODELS
We plan to use the auxiliary three-step mixture model approach. This approach will be automatically implemented and has the advantage of not changing the class membership with the inclusion of covariates. Baseline factors (T0) will be included in the growth mixture modeling (GMM) as auxiliary variables and their relationship with trajectory trajectories of loneliness will be tested using multinomial logistic regressions. All models will be estimated using Mplus 8.10.
STATISTICAL QUESTIONS
(1) What is the best way to handle the time-varying predictors of loneliness trajectories?
(2) What strategies can be employed to prevent over-adjustment in examining the predictors and trajectories?
(3) What approach would yield the least biased results when determining the optimal functional form of the trajectory over time?
(4) Are there alternative methods available for assessing the heterogeneous nature of loneliness beyond GMM?
REFERENCES
- https://www.washingtonpost.com/news/to-your-health/wp/2016/01/31/feeling-lonely-here-are-10-songs-that-know-just-what-thats-like/
- https://youtu.be/4WXYjm74WFI?si=W1_pm_59LPrpxGKi
- https://youtu.be/aMShwAnph8k?si=oRPaysQ6VKIQzbX5
- https://youtu.be/9XVdtX7uSnk?si=J0f8YIgFEmjIE_G8
- https://youtu.be/DFEOzbI8mA8?si=a_eoQ-9kroUmMrIJ
- https://youtu.be/4m3CMTeo-nU?si=p_h78X-IafyPiCbZ
DATE: Wednesday, 10 January 2024
TITLE: Introduction to Data Studio
AGENDA
- Introductions
- Syllabus
- Lecture
Alana O’Mara & Michael J. Gardner, Department of Medicine, Orthopaedics - Lower Extremity Orthopaedic Surgical Outcomes in Diabetic Females
Diabetes is an increasingly common disease in the United States, affecting around 13% of US adults. Diabetes can have systemic effects that impair bone mineral density such as increased release of cortisol and diabetic nephropathy which can lead to renal osteodystrophy. Furthermore, certain drugs commonly used in conjunction with diabetes can impact the skeleton. Thus, many diabetics have increased fracture risk. Moreover, post-operative surgery leads to derangements that can further exacerbate insulin resistance and lead to hyperglycemia which can lead to a relative immunodeficiency. Consequently, diabetics are more likely to experience post-operative adverse events. Very few studies have looked at the factors that play a role in 30-day postoperative outcomes for the study population of interest: female diabetics up to age 50 who have undergone lower extremity orthopaedic operations.
This study has two aims. The first aim is to compare the distribution of factors between two groups of female orthopaedic patients up to age 50 undergoing lower extremity surgeries: diabetics versus non-diabetics. The second aim is to determine which factors mentioned above play a role in post-operative outcomes and quantify the amount they may affect outcomes between those with and without diabetes. This study uses data from a large national surgical database that collects patient demographics, comorbidities, and 30-day postoperative outcomes. There are a total of 10,014 female subjects up to age 50 with lower extremity fractures. The specific factors of interest include: age, race, ethnicity, electiveness of surgery, fracture type, weight, history of COPD, use of medications, hypertension, congestive heart failure, dialysis, current cancer, race, smoking status, diagnosis of bleeding disorder, and transfusion before surgery. These factors are coded as either dichotomous (having disease or not), categorical (BMI, race, ethnicity), or continuous (weight and age). Postoperative outcomes we will consider include both continuous (length of hospital stay, days to death, days to unplanned reoperation or admission) and dichotomous (occurrence of superficial infection, occurrence of deep infection, occurrence of wound disruptions, occurrence of pneumonia, occurrence of intubation, occurrence of pulmonary embolism, occurrences of on ventilator, occurrence of renal insufficiency, occurrence of acute renal failure, occurrence of UTI, occurrence of stroke, occurrence of DVT, occurrence of MI, occurrence of sepsis, occurrence of death, unplanned reoperation or readmission).
Phase II Trial of Organ Preservation Program using FOLFIRINOX and Interval Long-Course Radiation for Rectal Cancer (INTERVAL-FOX)
INVESTIGATORS:
Thomas Lee Holden (1)
Michael J. Glover (1)
Erqi Pollom (1)
Judy Z. Fang (1)
(1) Department of Radiation Oncology
DATE: Wednesday, 6 December 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
In the United States, the standard treatment for locally advanced rectal cancer is preoperative chemoradiotherapy (CRT) followed by total mesorectal excision (TME). However, TME is associated with significant morbidity, including wound complications, sexual dysfunction, urinary retention, anastomotic leaks, and strictures. Therefore, in this study, we pursue an organ preservation approach using a total neoadjuvant approach of FOLFIRINOX (Chemo1) for 4 cycles followed by long-course radiation and then completion with FOLFIRINOX (Chemo2) for patients with non-metastatic, >T3 or low T2 rectal cancer.
KEY TERMS
Tumor-Node-Metastasis (TNM) Staging: T describes the size of the tumor, N describes whether the cancer has spread to the lymph nodes, and M describes whether the cancer has spread to a different part of the body. For this study, M0 means non-metastatic, T2 means the tumor has grown into the muscle layer of the rectal wall, and T3 means the tumor has grown into the outer lining of the rectal wall but has not grown through it.
OBJECTIVES
Primary: To assess clinical complete response (cCR) rate of an organ preservation approach using intensified chemotherapy with interval long-course RT.
Secondary: To assess safety in all enrolled patients, local regrowth rate, vcancer-specific time-to-event outcomes (disease-free survival, colostomy-free survival, and overall survival), longitudinal health-related quality of life of this organ preservation approach.
HYPOTHESIS
For overall patients, the null hypothesis for efficacy is a cCR of 0.2 versus an alternate cCR of 0.4. We assume an acceptable toxicity rate of ≤ 25% with an unacceptable toxicity rate of 40%.
STUDY DESIGN
Originally, we planned to design a single-arm, open-label, non-randomized study using the optimal Simon two-stage design method based on the above hypothesis. However, according to the clinical data for a similar study, we found that stage T4 patients might have lower cCR rate than stage T3 or less. Hence, except the original whole group study, we would also like to have the study stratified into two (2) groups and analyzed separately. This would allow a larger total number of patients into the study with two groups: patients staged T4 in one statistical group versus those with T3 or less. The T3 or less group would still have a historic cCR of 20% and a favorable expected outcome of 40% or greater. For the high-risk group with T4 initial thoughts would be a historical or unfavorable outcome of 10% with a favorable expected outcome of at least 20%.
STATISTICAL QUESTIONS
(1) For the case with 2 separate groups, would we still be able to use the Simon’s two-stage design method to calculate the sample size if we’ll have enough enrolled patients? Why or why not?
(2) If we can still use the Simon’s two-stage design, how to calculate the toxicity stopping/decision rule for the interim and end of the study analyses based on the given toxicity rate?
(3) If we can’t use the Simon’s two-stage design, what methods would be appropriate?
Cardiac Events after Radiation of Chemotherapy in Breast Cancer Patients
DATE: Wednesday, 29 November 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
INVESTIGATORS:
Scott Jackson (1)
Michael Binkley (1)
- Department of Radiation Oncology
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
This observational study consists of two patient groups: the treatment group receives combined radiation with Chemotherapy (XRT+Chemo) and the control group receives Chemotherapy (Chemo). Our project concerns competing risk regression for cardiac events. Death is a competing risk. Some of the covariates of interest only apply to the XRT+Chemo patients, namely, those related to radiation.
HYPOTHESIS & AIM
What is the risk for breast cancer patients of cardiac events after either XRT+Chemo or Chemo?
DATASET
The dataset includes 228 breast cancer patients treated at Stanford with either XRT+Chemo (treatment, n=174) or Chemo (controls, n=54).
STATISTICAL MODELS
We have fitted the following models to the dataset:
- Kaplan-Meier curves for comparing overall survival between Chemo and XRT+Chemo cohorts
- Fine-Gray curves for comparing cumulative incidence of cardiac events (using first event if multiple) with death as a competing risk.
- A set of univariable competing risk regression models was also utilized for a large set of covariates, with group (Chemo or XRT+Chemo) considered as a clustering variable.
ADJUSTMENT FOR BIAS
For these radiation covariates (collectively called X), just setting the value to zero for X in the control arm may not necessarily be a good approach. If X predicts the survival response for the treatment arm (suppose that is the case and that is why you want to include them in the covariates), you may want to see if other covariates available in both arms can predict X in the treatment arm. If they can, you may want to impute the missing X in the control arm to reduce the bias. An example was a recently finished trial in which patient satisfaction with the tool immediately after the intervention is highly predictive of the final outcomes. Of course, satisfaction with the tool can be collected only in the intervention arm and itself is a trial outcome (i.e., mediator). Several baseline covariates could predict patient satisfaction with the tool in the treatment arm. The investigators used a predictive X using the equation derived from treatment arm and applied Xhat to both arms and found interactions between Xhat and treatment arms in one of the two co-primary endpoints. It turned out certain patients were more likely to satisfy the treatment and often had better response than those unlikely to satisfy the treatment. We just want to show how to impute the unmeasured covariates depends on the nature of this study.
STATISTICAL QUESTIONS
The question concerns competing risks in time-to-event analysis with covariates that are not measurable in one arm.
- Is the use of a cluster term appropriate for treatment?
- How does one decide between cluster or frailty in these models, when we assume outcomes within a given cohort are correlated in some way?
- I tried using both cluster() and frailty() and the results were similar.
- Therneau and Grambsch discuss the differences between cluster() and frailty() as follows in Modeling Survival Data, Extending the Cox Model (pp. 169-170):
- Random effects or frailty model, such as that described in Oakes [119]. The model includes a random per-subject effect; multiple outcomes are assumed to be independent conditional on the per-subject coefficient.
- A marginal models approach. This has much in common with the generalized estimating equations (GEE) approach of Zeger, et al. [168]. (Referring to cluster)
- It was suggested to set radiation-specific variables (which are all numeric) to 0 for Chemo patients.
- Is this appropriate?
- Why or why not?
Data Studio Office Hour
DATE: Wednesday, 15 November 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION:
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
Data Studio Office Hour
DATE: Wednesday, 1 November 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
Red Teaming Generative AI in Healthcare
DATE: Wednesday, 25 October 2023
TIME: 3:00–6:00 PM (Students may leave at 4:20 PM but are welcome to stay.)
LOCATION: Room E241, CHEM-H Building (Bldg. ID 14-220), 290 Jane Stanford Way, Stanford, CA (See attached PDF with a map of building and location of room.)
WEBPAGE: https://dbds.stanford.edu/event/workshop-on-genai-in-healthcare-red-teaming/
ABSTRACT
Our BMDS 232 (Data Studio) Workshop on Wednesday, 25 October, will be a joint session with the Biomedical Data Science Generative AI Workshop. Enrolled students must attend the workshop in person during the regularly scheduled class time (3:00 to 4:20 PM) but are welcome to stay for the entire workshop.
DESCRIPTION
Please join us for an interactive session to test GenAI models for potential issues with biases, inaccuracies, and other matters related to healthcare. Red-teaming is a form of evaluation that elicits model vulnerabilities that might lead to undesirable behaviors. We will be looking for such behaviors on healthcare-related tasks. We will break into groups with table leaders from Stanford Healthcare, School of Medicine, CS and external partners providing technical and clinical insights. At the end we’ll have a read-out of findings and then continue the conversations during happy hour.
SCHEDULE
3:00pm | Check in begins
3:15pm | Table groups begin Red Teaming
4:45pm | Happy hour
6:00pm | Event concludes
__________________________
Data Studio Office Hour
DATE: Wednesday, 18 October 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
REGISTRATION FORM: https://redcap.stanford.edu/surveys/?s=WMH74XCX33
DESCRIPTION
The Data Studio Office Hour brings together a series of biomedical investigators with a group of experts for brief individualized sessions to solicit advice about a statistical and study design issue that arises while planning or conducting a research project.
This week, Data Studio holds office hours for your data science needs. Biomedical Data Science faculty are available to provide assistance with your research questions. If you need help with bioinformatics software and pipelines, check out the Computational Services and Bioinformatics Facility (http://cmgm-new.stanford.edu/) and the Genetics Bioinformatics Service Center (http://med.stanford.edu/gbsc.html).
Reserve a Data Studio Office Hour session by completing the Registration Form. Sessions are about 30 minutes long but might be extended at the discretion of the coordinator. If you register for a session, please be present at the start time on Wednesday.
If you are not able to register for a session, you are welcome to complete our Data Studio Consultation services form for a free one-hour meeting with one of our statisticians. You will find a link to the Consultation services form on our Data Studio web page (https://dbds.stanford.edu/data-studio/).
A Novel Chest Computed Tomography Scoring System in Children and Adolescents with Rheumatologic Diffuse Lung Disease
DATE: Wednesday, 11 October 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
INVESTIGATORS:
Beverley Newman (1)
Michal Cidon (2)
Terry Robinson (3, Presenter)
Paul Iskander (4)
Paul J. Thacker (5)
Evan Zucker (1)
Tzielan Lee (6)
Lu Tian (7)
Rex Moats (3)
(1) Pediatric Radiology, Stanford Children’s Hospital
(2) Pediatric Rheumatology, Children’s Hospital, Los Angeles
(3) Pediatric Radiology, Children’s Hospital, Los Angeles
(4) Pediatric Radiology, UCLA Mattel Children’s Hospital, Los Angeles
(5) Pediatric Radiology, Mayo Clinic, Rochester, Minnesota
(6) Pediatric Rheumatology, Stanford Children’s Hospital
(7) Biomedical Data Science, Stanford University School of Medicine
WEBPAGE: http://med.stanford.edu/dbds/resources/data-studio.html
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
INTRODUCTION
Pulmonary involvement in pediatric rheumatologic disease is associated with long-term high morbidity and mortality, yet current management is challenging because there are no current standardized approaches to defining, diagnosing, and providing risk stratification in assessing the extent and severity of diffuse lung disease in pediatric rheumatology patients with pulmonary compromise. In addition, while chest CT findings can predict the extent and severity of lung disease in pediatric rheumatology patients earlier than pulmonary function tests and 6-minute walk tests which are usually abnormal when patients become symptomatic, there are no current clinical approaches that systematically evaluate these patients with clinically acceptable chest CT imaging protocols.
There is currently limited chest CT imaging information in pediatric rheumatology patients, based on either clinical case reports or limited chest CT scoring primarily in adults and one study in children who were assessed for systemic sclerosis.
HYPOTHESIS & AIM
Development of a pediatric rheumatologic chest CT scoring system will represent a major advance in the understanding of early and progressive pulmonary findings in children with specific rheumatologic diseases that are associated with pulmonary complications. We hypothesize that a pediatric-specific rheumatologic scoring system for diffuse lung disease, will identify lung parenchymal findings associated with early and progressive lung disease. The purpose of this project was to establish a robust chest CT scoring system using inter-observer and intra-observer agreement of several chest CT imaging markers of diffuse lung disease to detect active and chronic progressive pulmonary changes in pediatric patients with different rheumatologic conditions. To develop such a scoring system, a previous adult Systemic Sclerosis Interstitial Lung Disease Scoring system developed by Golden and associates (Chest, 2007) was modified and adapted for a variety of lung conditions associated with different pediatric rheumatologic diseases.
We anticipate this pediatric diffuse lung disease score will be used to monitor treatment effects as well as being used as a clinical validation tool for further quantitative chest CT imaging analysis using currently developing deep learning algorithms for chest CT evaluation of diffuse interstitial lung disease in pediatric patients.
DATASET
We have curated one hundred twenty (120) chest CT scans obtained over a 10-year period (2011–2020). Three groups are included: (A) Disease Group (DG, N=42) of pediatric rheumatology patients with defined pulmonary involvement; (B) Disease Control Group (DCG, N=34) of pediatric rheumatology patients with no defined pulmonary disease; and (C) Normal Control Group (NCG, N=44) of age-matched normal control subjects.
METHODS
This study is the largest imaging comparison of DG, DCG, and NCG. The chest CT scans in our dataset were initially scored by three (3) board-certified pediatric radiologists with Certificates of Added Qualifications (CAQ) and 5–10 years of experience reading thoracic chest CT scans. All scoring was done after initial training with a pediatric thoracic radiologist with greater than 30 years of experience reading thoracic chest CT scans and pediatric pulmonologist with greater than 25 years of experience evaluating chest CT imaging, who developed the Pediatric Rheumatologic Diffuse Lung Disease Score [PRDLDS]. All pediatric radiology scoring was done by the 3 pediatric radiologists who were blinded to the clinical cases, clinical disease, and duration of findings.
After initial chest CT scoring evaluation in the N=120 scans by the three (3) pediatric radiology scorers, the PRDLD score was modified (PRDLD Score à mPRDLD score) to address inconsistent findings due to technical limitations of the majority of chest CT scans (non-contrast chest CT scans) or no specific adult findings that were not seen in pediatric patients. To further evaluate inter-reader reliability, after more extensive training using the mPRDLD score, the same 3 pediatric radiologists re-scored N=60 scans (DG: N=30; DCG: N=20; NCG: N=10) of the original N=120 scans 10 months later. To further address intra-reader reliability, N=30 scans (DG: N=20; DCG: N=10; NCG: N=5) of the 60 scans were further scored 4 months after completion of the N=60 scoring. In each re-scoring assessment, all de-identified scans were again randomized prior to reader evaluation and scoring.
In collaboration with Imbio, Inc., a CT image processing company, N=95 (N=42 DG subjects; N=33 DCG subjects; & N=20 NCG subjects) of the N=120 cases have been further utilized for a joint CHLA-Imbio, Inc. NIH SBIR Phase I research project for developing a deep learning (neural network) application for quantitative pediatric interstitial lung disease evaluation (Lung DeepLTA). We plan to compare the clinical scoring results from the mPRDLD Scores with that of the quantitative scores generated by Imbio Lung DeepLTA. In addition, we also have an internal funded CHLA research project evaluating standard lower dose chest CT and ultra-low dose chest CT in pediatric rheumatology patients at CHLA for the development of ultra-low dose chest CT imaging for serial pediatric rheumatologic assessment of early and progressive pulmonary disease in these patients.
GOALS
We hope to validate the current Pediatric Rheumatologic Diffuse Lung Disease Score. We have utilized an initial scoring assessment of subcomponent scores and modified scoring components based on initial scoring findings. Utilizing our inter-rater reliability and intra-rater reliability assessments, we hope to validate this new scoring system. Ultimately, we are interested in comparing the currently developing deep learning quantitative chest CT measurements (Lung DeepLTA) with the clinical imaging scoring system (mPRDLDS) we have developed for pediatric rheumatologic diffuse lung disease.
STATISTICAL QUESTIONS
(1) What is the best method for validating our clinical scoring system (mPRDLDS)? What are the best statistics we can use for validating a new clinical scoring system for a manuscript we are submitting to Pediatric Rheumatology? Given no gold standard, we will need good internal validation of the scoring system, and a means to address both accuracy and precision.
(2) Given limitations in the small numbers of subjects in certain pediatric rheumatology disease groups, what statistics can we use?
(3) We have a scoring system that provides regional assessment of disease extent/severity in six (6) lobar regions. What are the best statistics to use for demonstrating regional findings for each type of pediatric rheumatology disease? (Upper lobe vs. lower lobe predominance) differences in lobe distribution: RUL, RML, RLL, LUL, Lingula, LLL.
(4) What are the best statistical methods to compare clinical chest CT scores versus Lung DeepLTA findings? How can we best develop statistical analysis for DeepLTA findings for the different pediatric rheumatologic diseases that have similar or different lung diseases?
Clinical Trial Design for Glaucoma Treatment Using Humphrey Visual Field as Primary Outcome
INVESTIGATORS:
Laurel Stell, Biomedical Data Science
Jeffrey Goldberg, Ophthalmology
Gala Beykin, Ophthalmology
DATE: Wednesday, 4 October 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
ABSTRACT
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
Introduction
Glaucoma treatments are typically assessed by whether they control interocular pressure (IOP), but the disease often continues to progress despite reduction in IOP. The Humphrey Visual Field (HVF) exam, which measures the retina’s sensitivity to light, is widely used to diagnose glaucoma and its progress, but its measurement error can be large in comparison to the rate of progression. Consequently, estimating the rate of decrease in HVF measurements by linear regression generally requires regular exams over 10 years or more, and even then the slope is often not statistically significant. Finally, treatments are not likely to reverse damage but only slow or delay neurodegeneration. All of these factors can result in prohibitively large sample sizes or long trial times when using HVF as primary outcome in a clinical trial.
Hypothesis & Aim
We have performed exploratory analysis of HVF exams. We hope to leverage such data to improve clinical trial inclusion criteria and statistical tests for treatment effect.
Dataset
We have HVF data from a variety of sources: (a) thirty glaucomatous eyes in a test-retest study that performed weekly exams for three months (Artes et al, 2014), (b) data from Phase 1b trials including six or fewer exams over a year or two from about 150 eyes (Goldberg et al, 2022), and (c) the public UW-HVF data set of thousands of eyes, including 450 with at least nine exams over 10 years or more–but without clinical information such as diagnosis, progression or treatment.
Statistical Models
The HVF exam measures sensitivity at an array of 52 points on the retina. We will discuss properties of the measurements at individual locations, averaged over the whole retina, and averaged over each of six regions identified by mapping neurons in the retina. We are seeking advice on statistical models for testing treatment effect.
STATISTICAL QUESTIONS:
- Do we have sufficient pilot data?
- If not, what do we need?
- How to estimate power for possible outcome measures?
A Guide for the Statistically Perplexed
DATE: Wednesday, 27 September 2023
TIME: 3:00–4:30 PM
LOCATION: Conference Room X399, Medical School Office Building, 1265 Welch Road, Stanford, CA
INSTRUCTORS:
Ying Lu
Chiara Sabatti
Lu Tian
Balasubramanian Narasimhan (Naras)
Brad Efron
Mei-Chiung Shih
John S. Tamaresis
WEBPAGE: https://dbds.stanford.edu/data-studio/
ABSTRACT:
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project.
This will be the first meeting of the Autumn Quarter. Our agenda will include:
- Faculty and student introductions
- A surprise topic (pending approval)
- Introduction to the art of statistical consultation
Winter 2022 Studios
Abstracts, when available, are included in the drop down
Alana O’Mara & Michael J. Gardner, Department of Medicine, Orthopaedics - Lower Extremity Orthopaedic Surgical Outcomes in Diabetic Females
Diabetes is an increasingly common disease in the United States, affecting around 13% of US adults. Diabetes can have systemic effects that impair bone mineral density such as increased release of cortisol and diabetic nephropathy which can lead to renal osteodystrophy. Furthermore, certain drugs commonly used in conjunction with diabetes can impact the skeleton. Thus, many diabetics have increased fracture risk. Moreover, post-operative surgery leads to derangements that can further exacerbate insulin resistance and lead to hyperglycemia which can lead to a relative immunodeficiency. Consequently, diabetics are more likely to experience post-operative adverse events. Very few studies have looked at the factors that play a role in 30-day postoperative outcomes for the study population of interest: female diabetics up to age 50 who have undergone lower extremity orthopaedic operations.
This study has two aims. The first aim is to compare the distribution of factors between two groups of female orthopaedic patients up to age 50 undergoing lower extremity surgeries: diabetics versus non-diabetics. The second aim is to determine which factors mentioned above play a role in post-operative outcomes and quantify the amount they may affect outcomes between those with and without diabetes. This study uses data from a large national surgical database that collects patient demographics, comorbidities, and 30-day postoperative outcomes. There are a total of 10,014 female subjects up to age 50 with lower extremity fractures. The specific factors of interest include: age, race, ethnicity, electiveness of surgery, fracture type, weight, history of COPD, use of medications, hypertension, congestive heart failure, dialysis, current cancer, race, smoking status, diagnosis of bleeding disorder, and transfusion before surgery. These factors are coded as either dichotomous (having disease or not), categorical (BMI, race, ethnicity), or continuous (weight and age). Postoperative outcomes we will consider include both continuous (length of hospital stay, days to death, days to unplanned reoperation or admission) and dichotomous (occurrence of superficial infection, occurrence of deep infection, occurrence of wound disruptions, occurrence of pneumonia, occurrence of intubation, occurrence of pulmonary embolism, occurrences of on ventilator, occurrence of renal insufficiency, occurrence of acute renal failure, occurrence of UTI, occurrence of stroke, occurrence of DVT, occurrence of MI, occurrence of sepsis, occurrence of death, unplanned reoperation or readmission).
Jessica Hinman & Lorene Nelson, Epidemiology and Population Health - Trajectory Analysis of Multiple Sclerosis Disease Course
Multiple sclerosis (MS) is the most common inflammatory neurological disorder in young adults, affecting approximately 288–309 individuals per 100,000 in the US as of the 2010 census. While nominally separated into clinical subtypes on the basis of pathological features indicating a primarily autoimmune (relapsing-remitting) or neurodegenerative (progressive) disease process, there is a high level of disease course variability both across and within these categories. Developing a clearer understanding of multiple sclerosis disease course, and the extent to which the underlying determinants of that disease course are modifiable, requires first determining whether there exist distinct, identifiable disease trajectories. To that end, this study will utilize clinical measures relating to key functional domains of MS disease course including gait and upper extremity disability, cognitive decline, and relapse frequency.
The data were obtained from the Multiple Sclerosis Outcome Assessments Consortium (MSOAC) data platform which has compiled data from the placebo arms of 9 distinct clinical trials for a total of 2,465 individual participants. Because this data source was originally formed with the goal of developing and evaluating novel clinical measures of MS disability and progression, the trials included in the consortium extensively utilize standardized and validated prognostic and outcome metrics. The goals of our analyses will be to identify (1) whether distinct trajectories exist in our sample of longitudinal clinical measures, and (2) the extent to which any identified clusters correspond to the patients’ clinically assigned disease subtype.
Ryuji Uozumi, Department of Biomedical Data Science, Stanford, and Department of Biomedical Statistics and Bioinformatics, Kyoto University Graduate School of Medicine, Kyoto, Japan - Inverse probability of treatment weighting with time-to-event outcomes
Oxaliplatin, a third-generation platinum agent, is a key drug for chemotherapy in patients with colorectal, pancreatic, and gastric cancer. The major toxicity and/or adverse reactions induced by oxaliplatin include severe chronic neurotoxicity, which is observed in 44% to 50% of patients and also impairs the patients quality of life. My collaborator hypothesized that inhibition of the reninangiotensin system (RAS) may produce a preventive effect on oxaliplatin-induced neuropathy and performed a retrospective observational study to clarify whether RAS inhibitors prevent oxaliplatininduced peripheral neuropathy.
The primary end point was the time to first incidence of severe peripheral neuropathy at any point during or after the administration of oxaliplatin. To account for the effect of potential confounding factors, a multivariable Cox proportional hazards model was performed to estimate the difference between the RAS and non-RAS groups. Furthermore, to assess the robustness of the result in this observational study, inverse probability of treatment weighting (IPTW) using the propensity score was considered to estimate causal effect of the RAS treatment.
Jessica Brodt (Presenter), Ban Tsui, Quentin Baca, and Mastoora Nasiri, Anesthesiology, Perioperative and Pain Medicine - Analyzing Data from the RACER Clinical Trial
Adequate perioperative analgesia is essential for best patient recovery and outcomes. Current analgesic techniques for cardiac surgery rely primarily on opioids, which are associated with significant adverse effects in multiple organ systems, potentially increasing patient morbidity and complications.
The erector spinae plane (ESP) block is a relatively new anesthesia technique performed by injecting local anesthetic into the interfascial plane between the erector spinae muscle and the transverse process. Bilateral thoracic ESP blocks and catheters, combined with a general anesthetic, have been described as effective regional anesthesia for cardiac surgery, may provide opioid-sparing effects, and may improve pain and recovery after surgery.
The RACER (Regional Anesthesia for Cardiothoracic Enhanced Recovery) study was designed as a double-blind, randomized, placebo-controlled trial in cardiac surgery patients undergoing sternotomy to determine if bilateral ESP catheters improve postoperative recovery parameters. At this stage we have complete data for 28 patients randomized to treatment arm and 32 patients randomized to placebo arm (pre-study power analysis needed 18 per group).
Our primary aim was to determine if local anesthetic via ESP catheters (treatment) reduces opioid requirements compared to patients receiving normal saline via ESP catheters (control). Secondary aims were to determine if local anesthetic via ESP catheters reduces pain scores, duration of mechanical ventilation, time to return of bowel function, and length of stay (LOS), or favorably shifts levels of pro- and anti-inflammatory biomarkers.
Vikram Fielding-Singh, Department of Anesthesiology, Perioperative, and Pain Medicine; Anson Lee, Department of Cardiothoracic Surgery; & Steven Borkan, Renal Section, Boston University Medical Center - Biomarker of Acute Kidney Injury for Cardiothoracic Surgery Patients
Cardiac surgical patients are at high risk for acute kidney injury (AKI) due to preexisting kidney dysfunction, hemodynamic instability, and the use of cardiopulmonary bypass. Although the initial kidney injury likely occurs in the operating room, current clinical criteria (urine output and serum creatinine) often will not make the diagnosis until post-operative day 1 or 2. Nucleophosmin (NPM) is an intracellular protein that becomes phosphorylated (p-NPM) during ischemic stress and causes cell death of proximal tubular epithelial cells in the kidney. We have previously developed NPM and p-NPM as a marker for AKI and as a therapeutic target in animal models of renal ischemia. We now plan to evaluate its use in humans.
This is a prospective cohort study of patients undergoing cardiothoracic surgery at moderate to high risk of AKI. We will gather urine samples intra- and post-operatively. Samples will be analyzed for urine NPM and p-NPM, common commercially available AKI diagnostics (i.e., Kim-1, NGAL, NephroCheck), and urine creatinine. Our primary outcome of interest will be AKI as diagnosed by established KDIGO criteria up to postoperative day 5.
We have three specific aims. Aim 1 will characterize the kinetics of urinary NPM and p-NPM in cardiothoracic patients at high risk of AKI. Aim 2 will construct a prediction model using urinary NPM, p-NPM, and the p-NPM-to-NPM ratio to predict AKI using currently accepted KDIGO criteria. Aim 3 will compare performance of urinary NPM and p-NPM to currently available urinary diagnostics (Kim-1, NGAL, and NephroCheck) to predict AKI. The kinetics and concentrations of NPM and p-NPM in human urine are currently unknown. Thus, we plan to address Aim 1 first to generate preliminary data that will be used to finalize the design of the study used to achieve Aims 2 and 3.
Aubrey Roberts, Stanford Healthcare Innovation Lab, Snyder Lab, Department of Genetics - Access to COVID-19 Testing and Resources as Predictors of Mental Health
The COVID-19 pandemic continues. Previous research has shown that mental health is impacted by factors such as quarantine and lockdowns. Poor mental health may persist as a long-term consequence of COVID-19 diagnosis. However, it is unclear which factors are protective against the development of mental health disorders during the pandemic. With the onset of rapid testing, consumers are able to test more frequently and have greater availability of testing. Does this make consumers feel safer or improve their mental health?
The goal of this study is to understand how COVID-19 support resources—access to rapid testing, frequency of testing, and perception of available resources after testing positive—impact mental health and whether these could be protective factors against the development of mental health disorders. We have three primary hypotheses: 1. Frequency of testing—People who test daily will have lower distress scores than those who test less frequently 2. Accessibility of tests—People with higher perceived accessibility to rapid tests will have lower distress scores than those who dont feel they can access rapid tests 3. Resources (for people testing positive only)—People with higher perceived access to resources will have lower distress scores than those who felt they could not access resources
Stanford University is partnering with Intrivo On/Go Rapid Antigen Testing to conduct a cross-sectional survey study of existing consumers in Intrivos database. The survey will have three parts: 1. Demographics 2. Mental health (K10 questionnaire) 3. Survey questions on frequency of testing, perceived availability of testing, and (only for participants who have tested positive) access to COVID-19 resources after testing positive.
We hope to learn more about what factors can protect against or mitigate the development of mental health disorders during the COVID-19 pandemic, with specific focus on frequency and availability of COVID-19 testing and perception of available resources after testing positive. If we understand what factors might protect against worsening mental health during the pandemic, then we can work with policymakers to help implement changes and focus on scaling up these resources to reduce the burden of mental health disorders at a population level.
Fall 2022 Studios
Abstracts, when available, are included in the drop down
Theresa Lii, MD, and Boris Heifets, MD, PhD, Anesthesiology, Perioperative, and Pain Medicine - RCT of Intraoperative Ketamine vs Saline in Depressive Surgical Patients
This is a single-site, double-blinded, randomized clinical trial (RCT) to evaluate the antidepressant superiority of intravenous (IV) ketamine compared to placebo when administered during surgery to adult patients with symptomatic major depressive disorder. Participants are randomly allocated in a 1:1 ratio to one of two groups: Group A (n=20) will receive a single administration of IV ketamine during surgery. Group B (n=20) will receive IV saline (placebo) during surgery. The study drug will be given after anesthetic induction to ensure participant blinding. Healthcare providers, investigators, and outcomes assessors are also blinded. Our primary outcome measure is the Montgomery-Asberg Depression Rating Scale (MADRS), which is widely used in depression trials. Baseline MADRS scores are obtained from all participants. Post-intervention MADRS scores are collected on post-operative days 1, 2, 3, 5, 7, and 14. Secondary outcomes include the Hospital Anxiety and Depression Scale (HADS), pain scores, opioid use, and hospital length of stay. We have reached three-quarters of our enrollment goal. Data has been collected on these participants. We have blinded data available for review. Our goal is to finalize our statistical analysis plan prior to unblinding of data.
Patrick DeMoss, Department of Pediatrics, Division of Hematology-Oncology - Probability of Leukemia Subtypes Given Clinical Variables
In certain contexts, it is not possible to easily ascertain the particular type of leukemia when viewing it under the microscope. For emergency situations, not knowing the diagnosis can delay initiation of life-saving treatment, leading to catastrophic consequences. Given clinical variables such as age, presence/absence of a mediastinal mass, and development of coagulopathy, is it possible to derive probabilities (and their uncertainties) of a particular type of leukemia? I use a collection of published data to estimate probabilities for clinical variables and disease incidence. Because I am uncertain of their underlying distributions, I use bootstrapping with 10,000 repetitions to derive 5% & 95% credible intervals for my parameters. I calculate the point estimate of the disease probability given clinical parameters using Bayes Theorem with the help of a tree diagram. Furthermore, I will calculate 5% & 95% credible intervals for the disease probability itself, using a parametric bootstrapping package in R called bootComb.
Manisha Desai, Derek Boothroyd, & Isabel Weng, Quantitative Sciences Unit - Estimating Lab-performance Adjusted Incidence Rate
The project originates from a clinical study that QSU has been collaborating on. It is a longitudinal cohort study that the primary goal is to evaluate the prevalence and incidence of sars-cov-2 infection in the 6 bay area counties. We designed a sampling framework to randomly draw participants from bay area counties using census track data. We created a combined weight variable for each participant to account for both sampling frameworks and non-response bias. Participants in our study were brought up for a baseline visits and up to 6 monthly follow up visits. During the visits, participants had a swab for rt-PCR testing as well as a blood draw for serology testing. Since the performance of serology tests were not ideal and we did not have very frequent follow-up for us to capture all acute infections, we therefore planned to adjust for the lab-performance in our estimates of prevalence and incidence. We also hoped to incorporate the weights into our point and variance estimates for generalizability purpose. We developed a MLE-based approach to estimate incidence and prevalence simultaneously and used bootstrapping to estimate the corresponding confidence intervals. However, our method relies on strong assumptions, which includes 1) constant incidence over time; 2) the weight variable is a fix number for each participant; 3) discrete and finite number of follow up visits with fixed gaps between visits (e.g. monthly, weekly visits); 4) lab performance (sensitivity, specificity) did not change across visits.
Linda Anh Nguyen and Elisa Karhu, Department of Medicine, Division of Gastroenterology - Barriers to Lifestyle Change in Irritable Bowel Syndrome
Irritable bowel syndrome (IBS) is a chronic condition that impacts approximately 6% of the population. Symptoms include intermittent abdominal pain associated with a change in bowel function or stool form. First-line treatment recommendations include diet and lifestyle modifications. This is a prospective survey study of IBS patients. The survey will be administered to patients in clinic as well as an internet survey. Typical IBS surveys have a response rate that ranges between 30% and 60% (median 35%). The race/ethnicity of study participants in prior IBS clinical trials and survey studies in IBS is typically 75% non-Hispanic White, 7% Black, 7% Latinx, 5% Asian, and 6% other. Similar studies do not exist; therefore, the effect size is not known to assist with sample size determination.
This study has two aims. The first aim is to understand barriers to various therapies including diet, sleep, mental health, herbal, and pharmaceutical therapies. The second aim is to compare the patient-perceived acceptability of different nonpharmacologic and pharmacologic interventions. Identifying barriers to treatment can help formulate strategies to improve adoption of lifestyle changes in the IBS population. Patients will be asked a series of questions regarding common therapies prescribed or recommended for IBS. The first question is a categorical (YES/NO). Patients who answer NO will be asked the same 14 questions regarding the reason why they gave that answer. For all patients in the study, we will collect demographic information (age, gender, ethnicity, language fluency, income, education), clinical variables (duration of disease, medical comorbidities), and treatment-specific response. The demographic and clinical variables will be assessed to determine if any of these factors are associated with any of the response categories.
Gopin Saini, Pediatrics-Stem Cell Transplantation; Alice Bertaina, Pediatrics-Stem Cell Transplantation; and Paul Grimm, Pediatrics-Nephrology - HSCT before RT for Patients with Genetic Disorders
Renal transplantation (RT) is the treatment of choice for eligible patients with end-stage renal disease. Shortand intermediate-term outcomes of renal allografts have improved due to fewer early rejections and to better standardized immunosuppressive treatment strategies. The induction of immune tolerance for the renal allograft is the ultimate goal in the field of RT to enhance long-term outcomes significantly. This is crucial for pediatric patients with genetic disorders because they need multiple RTs during their lifetime in the absence of immune tolerance.
We are planning a single-center, non-randomized, non-controlled, open-label Phase 1 trial. The study population will consist of pediatric-young adult patients requiring either a first or subsequent RT due to underlying genetic or immunologic disease. We will test a treatment modality consisting of alpha-beta-positive T-cell/CD19 B-cell depleted hematopoietic stem cell transplantation (HSCT) followed by RT from a mismatched related or unrelated donor. In this trial, dose-finding will not be needed because both the HSCT and RT are standard-of-care interventions, albeit for different indications. Our aim for each patient is to achieve full donor chimerism, perform RT with minimal immunosuppression (IS), and taper the IS quickly to withdrawal.
Based on the trial objectives, we have two primary endpoints: withdrawal of IS by Day +90 following RT; normal renal function in the absence of IS at 1 year. We will pause the trial if any of the following occur: a death related to HSCT; primary HSCT graft failure (we can tolerate up to 20% whereas the current rate is less than 10%); Grade III–IV acute GvHD (we can tolerate up to 20% whereas the current rate is less than 10%).
Ruben van Eijk (Department of Biomedical Data Science and University Medical Center Utrecht, Utrecht, the Netherlands) and Ying Lu (Department of Biomedical Data Science) - Estimating Penetrance of C9orf72 Repeated Expansion for Family Members of ALS Patients
Amyotrophic lateral sclerosis (ALS) is a rare neurodegenerative disorder. It leads to loss of motor neurons which causes severe muscle weakness. Patients usually die, on average, within three to five years after first symptom onset. The cause of ALS is largely unknown, but is believed to be a combination of genetic and environmental risk factors. In approximately 10% of the patients with ALS, a familial form of ALS can be identified where multiple family members are affected. The most common genetic mutation is a repeat expansion of the C9orf72 gene. It is found in 5–10% of the patients with ALS.
A key clinical question is how to counsel offspring and family members of patients who are known to be C9orf72 carriers. To date, there are only a few studies that have looked at the penetrance of C9orf72. Penetrance is defined as the probability for an individual to develop ALS if the same carries the gene. We have collected data on first-degree family members of patients with ALS who are known to be C9orf72 carriers. We would like to estimate the penetrance of C9orf72 and have used a binomial model.
Spring 2021 Studios
Abstracts, when available, are included in the drop down
Stephan Rogalla (1), Derek Holman (2), & Aaron Mayer (2). (1) Department of Medicine, Division of Gastroenterology & Hepatology. (2) Department of Radiology, Molecular Imaging Program. - High-dimensional Fluorescent Microscopy for Guiding Therapy in Ulcerative Colitis Patients
The unique characteristics of tissues arise from the identities of their constituent cells and how these cells interact and communicate. We use spatially-resolved high-dimensional fluorescent microscopy to uncover the spatial cellular organization of gut tissues from patients with Ulcerative Colitis. We are interested in using these tissue architectural themes to predict whether patients will respond to therapy. By representing our microscopy images as Voronoi tessellations and assigning fluorescence intensities to each polygon, we are able to readily extract both cell types and their spatial relationships. We then generate classifiers using machine learning algorithms and logistic regression.
Christian O’Donnell, Anesthesiology; Melanie D. Ashland, Stanford Cancer Institute; Connor O’Brien, Cardiovascular Medicine, UCSF; and Elena Vasti, Anesthesiology - Predictive Value of NT-pro-BNP as a Biomarker for the Severity and Survival from COVID-19 in a Nationwide Hospitalized Cohort
COVID-19 has transformed our world and presented one of the largest medical challenges of our generation to characterize, prognosticate, and treat. Older patients and those with risk factors for cardiovascular (CV) disease such as obesity, hypertension (HTN), diabetes (DM), and coronary artery disease (CAD) experience worse outcomes. Cardiac injury as measured by elevations in troponin and brain natriuretic peptides (BNP) such as the N-terminal proBNP (NT-proBNP), are associated with a higher risk of mortality in patients hospitalized with COVID-19. NT-proBNP is an established biomarker for diagnosing and monitoring heart failure, ischemic heart disease, and myocardial injury. NT-proBNP also carries prognostic value in lung diseases where elevations have shown to predict cardiopulmonary death and risk of exacerbations in patients with chronic obstructive pulmonary disease (COPD) without a history of HF. However, NT-proBNP is not always routinely checked in clinical practice for admissions related to COVID-19. There is limited literature on the use of NT-proBNP for predicting clinical outcomes in COVID-19. We theorize that COVID-19-related lung injury may be causing cor-pulmonale to elevate NT-proBNP levels, which may carry predictive value. Our goal is to better define the relationship between NT-proBNP and clinical outcomes in hospitalized patients, to assess the predictive value of NT-proBNP as a biomarker for the severity and survival from COVID-19.
Bethlehem Mekonnen & Charles Lin, Department of Ophthalmology - Clinical Differentiation of Corneal Ulcers and Scars
Among corneal diseases, microbial keratitis is the most common cause of corneal blindness and one of the true ocular emergencies leading to vision loss within hours if left untreated. An approach to diagnose and guide management of corneal ulcers remotely could make a significant impact in vision outcomes, especially for patients with limited access to eye care. We aim to evaluate the diagnostic accuracy and reliability of ophthalmologists of various sub-specialties and training levels to detect the activity of corneal ulcers using slit-lamp photographs.
We have prepared an electronic survey tool containing anterior segment slit-lamp photos of corneal findings from patients with gold-standard diagnosis of microbial keratitis or corneal scar. The participants, recruited from Stanford ophthalmologists, will classify each photos into one of the following three categories: active corneal infection, scar, or unsure. We will stratify the survey results by training level and sub-specialty of the grader to determine accuracy, sensitivity, specificity, and reliability with weighted kappa statistics.
Melissa Mavers, Pediatrics, Stem Cell Transplantation - Suppressing GvHD via Immune Tolerance
Allogeneic hematopoietic stem cell transplantation (HSCT) plays a vital role in treating high-risk hematologic malignancies and some non-malignant conditions. However, many patients undergoing HSCT develop graft-versushost disease (GVHD), leading to substantial morbidity and mortality. Several studies have shown the significant role that invariant natural killer T (iNKT) cells, a type of innate lymphocyte, play in suppression of graft-versushost disease (GVHD). Importantly, murine studies have demonstrated multiple subsets of iNKT cells, including those with pro-inflammatory and immunosuppressive properties, and the subsets with the capacity to prevent GVHD have been identified. However, the heterogeneity of human iNKT cells remains poorly understood. My overall goal for this project is to define human iNKT cell heterogeneity and to develop strategies for targeted selection of immunosuppressive iNKT cells, with the future goal of initiating a clinical trial of adoptive transfer for GVHD prevention. My first aim is to define the heterogeneity of human iNKT cells at the transcriptomic level and identify which transcripts, particularly those which correspond to surface proteins, most significantly distinguish unique subsets of iNKT cells. This will allow for the design of a fluorescence activated cell sorting strategy to isolate distinct subsets and enable the subsequent aim of elucidating functional differences between subsets to identify that which is most immunosuppressive. To address the first aim, I will perform single cell RNA-Sequencing on isolated human iNKT cells from 4-6 different tissue sources and 2-3 donors per tissue source, using the BD Rhapsody targeted scRNA-seq platform as well as BD whole transcriptome assembly.
Sindy KY Tang, Department of Mechanical Engineering - uDicer: Micro-Dissection for Personalized Cancer Therapy
Patient-derived tumor organoids (PDO), involving the in vitro culture of fresh tumor fragments, have emerged as promising models for predicting patient drug response to personalize cancer therapy. PDOs recapitulate the tumor micro-environment, resemble the source tumor phenotypically and genomically, and are compatible with high-throughput drug screening. We have recently demonstrated a new type of PDO that cultures tumor fragments as a cohesive unit, allowing the in situ preservation of diverse immune cell types alongside tumor cells without artificial reconstitution. This approach has enabled the modeling of patient-specific responses to immune checkpoint inhibitors.
One of the first steps in the generation of PDOs is the dissection of patient tumor specimens into small fragments. Mechanical dissection is critical to preserving the in vivo association between tumor cells and endogenous immune and non-immune elements. Current mechanical dissection relies primarily on manual mincing of tumor specimens into small fragments. It results in fragments with a broad size range, is imprecise, and irreproducible. Fragments that are too small are unlikely to preserve cell type diversity, whereas fragments that are too large may suffer from inadequate nutrient supply and suboptimal oxygenation and viability.
There is an unmet need for a better way to generate tumor fragments of controllable, uniform size and to identify optimal size(s) to maximize tumor micro-environment preservation. We are designing the uDicer to mechanically dissect tumor specimens into uniform sub-millimeter fragments. We want to demonstrate increased uniformity of the size of viable PDOs compared with those prepared by manual mincing. We want to determine the relationship between fragment size and PDO viability, cell type diversity, and reactivity to immune checkpoint inhibition. Performance measures include fragment size uniformity, PDO viability, cell type diversity, and tumor-infiltrating lymphocyte reactivity.
Xuejun Gu and Rie von Eyben, Radiation Oncology - Predictive Model for Recurrent Brain Metastases
Advances in therapy of brain metastases (BMs) have improved overall survival to the extent that a portion of these patients may live long enough to experience recurrent BMs (rBMs). Care guidelines for rBMs are not well-defined. The complexity of rBMs makes it a challenge to manage rBMs because the current clinical practice environment lacks proper tools to identify them and generate a patient-specific optimal treatment plan. To address these needs in rBMs management, we propose to develop, validate, and translate an AI-based rBMs (AirBMs) management platform for safe and effective care. The proposed platform consists of three AI-based computation modules to conquer identified challenges in rBMs management: 1) Detector: a conventional and AI-combined imaging processor for rBMs detection/differentiation; 2) Predictor: a recurrent-neural-networkbased rBMs clinical outcome prediction using time-sequential multi-facet data; 3) Planner: an iterative clinical outcome-oriented plan optimizer. AirBMs will be developed on retrospective data and validated on prospective rBMs treatment. The prospective clinical validation will provide critical clinical knowledge and evidence as feedback to improve AirBMs performance. The ultimate goal of the project is to translate the AirBMs to routine clinical practice.
Winter 2020 Studios
Abstracts, when available, are included in the drop down
Larry Fu-nien Chu & Amy Price, Anesthesiology, Perioperative, and Pain Medicine - Infection Prevention and Control in Pandemic Conditions
This study will build on the World Health Organization Infection Prevention and Controls (WHO IPC) guidance to address infection and prevention control research gaps about the safety and efficacy of the source- and infection-control equipment used in the field during pandemic conditions. It will provide evidence for design improvement of existing infection-control strategies in order to use hospital equipment effectively in less-than-optimal conditions and will provide evidence concerning personal protective equipment (PPE) and the role of powered air-purifying respirators (PAPR) and their implementation during pandemic conditions. This study consists of three aims. The first aim addresses Human Factors Simulations. We will compare and test auditory and visual acuity plus cognitive load and error tracing across equipment combinations N95/face shield, Traditional PAPR, and Light PAPR. The second aim addresses Field Testing Applications. We will support the field studies in Bologna and Sao Paola and offer evidence for optimal PPE choices in specific pandemic environments and offer ways to compensate for unavoidable loss of dexterity, auditory or visual acuity on the field. The third aim addresses Aerosol Dispersion Evaluation. We will evaluate the dispersion of aerosol particles under various medical environments and aerosol generating procedures (AGP) to characterize and potentially risk stratify such environments and potential mitigating PPE.
Jenny Hong & Catalin Voss (Computer Science) & Kristin Bell (School of Law, University of Oregon) - The California Parole System
California is one of the epicenters of America’s mass incarceration crisis: 25% of its 115,000 state prisoners serve a life sentence. These individuals will die in correctional facilities unless released by the Board of Parole Hearings (BPH) with gubernatorial approval. Each year, BPH schedules thousands of parole hearings for eligible candidates, after which the candidates are either granted or denied parole for some number of years. In 2019 alone, BPH held 6,061 hearings and granted parole in 1,181 cases, a grant rate of 19.5%. The parole system has remained largely opaque, since the only public information it produces is a 150-page transcript of the 2+ hour free-form hearing dialogue. We have obtained a complete dataset of 35,000 parole hearing transcripts from the State of California dating from 2007 to 2019. In 2020, we sued the State of California to obtain the race and attorney representation data for all of the 15,766 prisoners covered by these transcripts. We are now attempting to construct the most complete picture to date of the California parole system by stitching together information from a number of sources: (1) covariates automatically extracted from the transcripts using Natural Language Processing (NLP) techniques and automated parsing of the PDF documents, (2) manually annotated information covering a subset of approximately 1,000 transcripts, (3) information scraped from California Department of Corrections & Rehabilitation websites, and (4) the results of our lawsuit. We are conducting a retrospective observational analysis seeking to describe the independent effect of approximately 50 covariates on the parole outcome (grant or deny). Most of these covariates are binary (e.g., Did the district attorney oppose release?), some are continuous (e.g., How many years ago was the candidates last disciplinary infraction in prison?), and a few are ordinal (e.g., Was the psychologists assessment one of high, medium, or low risk?)
Conrad Safranek, Biology - Detecting Pandemic Viral Variants with Rideshare Data
We are trying to demonstrate that COVID-19 diagnosis data merged with rideshare trip data may enable detection of novel, more infectious viral variants. We have developed Rideshare Infection Detection (RIDE), a mathematical model of rideshare vehicle transmission and analytical method for analysis of aggregated rideshare plus COVID-19 data. RIDE allows comparison of expected and observed infection numbers in the rideshare network, and thus can detect the infectivity of the current strain. Because aggregated rideshare plus COVID-19 data is not currently available, we create synthetic data via a simulation of viral propagation through Los Angeles with a hypothetical baseline viral variant A. We then analyze the results with RIDE, assuming either variant A or an alternative, incorrectly hypothesized, more infectious variant B. When analyzed with the true variant (variant A), the difference in the number of observed infections and the number of expected infections should be about 0. Our initial simulations suggest that, despite noise, analysis assuming variant A leads to results that are closer to 0 than analysis with variant B.
Marc Safran & Chris Jamero, Orthopaedic Surgery - HipSTER—Hip Surgery Treatment Evaluation Registry
The field of hip arthroscopy has been growing exponentially over the past several years. Both the UK and Denmark have hip arthroscopy registries. However, there is no such registry in North America. Our vision is to develop a hip arthroscopy registry to track pre-operative baseline measurements, intra-operative findings, and post-operative patient outcomes for up to 10 years. This will be a multi-site QA/QI initiative. Data will be collected from both patients and surgeons. We intend to use the data for future research projects.
Nancy Morioka-Douglas, Eunice Rodriguez and Ashini Srivastava - Stanford Youth Diabetes Coaches Program
We aim to demonstrate that, compared to controls, high school youth from disadvantaged, underrepresented communities will increase problem solving skills, health knowledge, self-efficacy, patient activation, healthy behaviors, and talking about health at home after participating in the 8-week Stanford Youth Diabetes Coaching Program (SYDCP). Over the past 10 years, we have developed, piloted, and evaluated SYDCP using quasi-experimental design with small convenience samples which, when aggregated, have shown statistically significant improvement in these measures. We are exploring the feasibility of using a cluster randomized trial with delayed intervention. We estimate that we could recruit up to 10 high schools (5 per year over 2 years or 10 in one year), each with 2 participating classes of approximately 20 tenth-grade students, which would yield 200 participants and 200 controls. Participants would complete the program in the Fall, while controls will complete the program in the Spring. We aim to have all participants complete validated surveys at 3 points in time: baseline (beginning of fall semester), after the intervention group completes training (end of fall semester), and after the control group completes training (end of spring semester).
Caitlyn Seim, Mechanical Engineering; Maarten Lansberg, Neurology; Allison Okamura, Mechanical Engineering - Comparison of Vibrotactile Stimulation Approaches on Symptoms of Spastic Hypertonia
Stroke survivors often have involuntary muscle contraction in their hand and arm (spastic hypertonia). Promising preliminary evidence suggests that vibrotactile stimulation may be associated with reductions in this condition. This project will measure the impact of four stimulation conditions. The study has a within-subjects design and each participant will experience four visits. A different stimulation condition will be applied during each visit. Symptoms of spastic hypertonia will be measured at three joints using two ordinal scales, two angle measures recorded using motion capture, and a custom tool. Measures will be taken at four timepoints, including before and after stimulation. Aim 1 is to evaluate which condition showed the greatest change in measures. Aim 2 is to evaluate change between each two time points within each condition, providing us data on the duration of effects.
Ruben van Eijk, Visiting Scholar, Department of Biomedical Data Science, and University Medical Center Utrecht, Utrecht, the Netherlands - Joint Modeling of Longitudinal and Time-to-event Endpoints in Clinical Trials
Time-to-event endpoints are often used to determine treatment efficacy in clinical trials. It is common practice to collect alongside the time-to-event endpoint additional longitudinal information on important biomarkers. Examples include the collection of prostate-specific antigen alongside time-to-death in prostate cancer trials, or fasting plasma glucose levels alongside time-to-diabetes in preventive clinical trials for type 1 diabetes. In many instances, the longitudinal biomarker could be seen as potential surrogate marker for the event of interest, and may provide additional insights in the treatment effect. In this project we use a joint modeling strategy to explicitly model the intrinsic relationship between the event and the biomarker by incorporating the longitudinal biomarker process into the hazard function of the event. In this framework, treatment could either affect the time-to-event endpoint through the biomarker, or treatment could act through a separate pathway that is not accounted for by the biomarker. Characterizing the different pathways and the total treatment effect are the parameters of interest. We will illustrate the approach using observed clinical trial data in amyotrophic lateral sclerosis, a rapidly progressive neurological disease with an average survival time of 18 months after diagnosis.
Fall 2020 Studios
Abstracts, when available, are included in the drop down
Matthew Muffly, Department of Anesthesiology; Fania Lazarov, Department of Pharmacy, LPCH - Accuracy of Administered Small-volume Opioid Injections in the Pediatric Post-operative Setting
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigators will discuss the following project with the group.
Post-operative pain management in pediatric patients requires intermittent administration of opioid medications that are available in concentrated form. Small weight pediatric patients (less than 20kg) are at a particular risk for receiving potentially inaccurate volumes of opioid medications given low milligram per kilogram dosing, lack of commercially available diluted formulations, and variability in administration techniques among providers. We hypothesize that specific administration techniques and the use of pharmacy compounded diluted opioid products is associated with greater accuracy of administered small volume opioid doses in the post-operative setting.
Beth Darnall, Director, Stanford Pain Relief Innovations Lab; Sean Mackey, Chief, Division of Stanford Pain Medicine - Transforming Pain Care in America—No Patient Left Behind
Each year pain costs the U.S. economy more than diabetes, cancer, and heart disease combined. Pain is ubiquitous across most health conditions, disproportionately affects women and minorities, and is the leading cause of disability. Pain is cited as the main reason people seek primary care, and for first use of illicit substances among people with addiction. Strikingly, behavioral pain treatment is largely inaccessible in primary care settings and addiction treatment programs. There is in urgent need for low-cost integrated technological infrastructure that can characterize the needs of each individual early on and deploy low-risk, scalable, tailored, and on-demand behavioral treatment.
The study design we are planning will be prospective, randomized-controlled, multi-site, multisetting, pragmatic, implementation research study that includes a subsequent responsive adaptive clinical trial design (N=1,200). We will provide free national access to an existing cloud-based learning health system (LHS) and treatment platform that will deliver on-demand and personalized digital treatments for acute and chronic pain. The LHS will be accessed via the internet. Any report of pain triggers an automatic invitation to enroll and all participants complete a common streamlined survey battery.
Lori Muffly, Assistant Professor, Blood & Marrow Transplantation; Evan Weber, Postdoctoral Fellow, Center for Cell Therapy - Phase I Study of KTE-X19 + Dasatinib in Relapsed/Refractory Adult Acute Lymphoblastic Leukemia
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
A substantial proportion of adults with B-cell acute lymphoblastic leukemia (ALL) will develop relapsed or refractory (r/r) leukemia. Outcomes for this population are poor. The development and recent FDA approval of chimeric antigen receptor T-cell (CART) therapy directed at CD19 for ALL has revolutionized the approach to this disease. However, no commercial CART product exists for r/r ALL in adults. Among the published single center clinical trials of CART in adult ALL, response rates are universally high; 50-70% will achieve complete response. However, at least two major barriers to progress stand out. One is CAR-mediated toxicities (cytokine release syndrome [CRS] and neurotoxicity) induced by the early and rapid expansion and proliferation of these cells. The other is subsequent T-cell exhaustion with loss of clinical response.
We screened several small molecule kinase inhibitors on CAR T-cell functionality and identified dasatinib, an FDA-approved drug for the treatment of Ph+ ALL and chronic myeloid leukemia (CML). It is a potent and reversible inhibitor of CAR T cell cytotoxicity, cytokine secretion, and proliferation. Dasatinib inhibits CAR T-cell functionality in vitro and in vivo at nanomolar concentrations similar to those detected in the serum of Ph+ ALL and CML patients treated with dasatinib. These data suggest that dasatinib could be safely used as an OFF switch to prevent or mitigate CAR-mediated toxicities.
In a separate study, we discovered that transient disruption of CAR signaling (i.e. ”rest”) via downregulation of surface CAR could reprogram exhausted CAR T cells to resemble memory-like cells, thereby leading to functional reinvigoration. We hypothesized that transient application of dasatinib could recapitulate these results by inducing ”rest”. Indeed, using an in vitro model of CAR T-cell exhaustion, dasatinib treatment of exhausted CAR T-cells for 4-7 days enhanced the expansion of CD8+ cells, decreased the expression of canonical exhaustion markers, and enhanced antigen-dependent cytotoxicity and cytokine secretion. Notably, repeated 3-day dasatinib pulses prolonged the anti-tumor response and enhanced survival in 2 separate dasatinib-insensitive tumor xenograft murine models. Tumor-infiltrating CAR T-cells in mice treated with dasatinib exhibited an increased percentage of memory-like cells and enhanced degranulation when re-stimulated ex vivo. Collectively, these results indicate that CAR T-cell and dasatinib combination therapy may result in enhanced safety and efficacy.
John S. Tamaresis, Biostatistician, Biomedical Data Science - Development of a Prediction Model for Unplanned Care Events
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
The Center for Medicare and Medicaid Services (CMS) has recently focused on unplanned care events in cancer patients as a measure of both the quality of care delivered and a source of potential cost savings. These events have appeared in a pay-for-reporting program that contains a metric, OP-35, which measures the rate of hospital admissions and emergency department visits in patients receiving outpatient chemotherapy. These chemotherapy-related events are felt to be potentially avoidable with appropriate access, outreach, and preventative measures.
For practices with very large patient populations such as academic medical centers, generic interventions to address unplanned care can quickly overwhelm available resources. Focused interventions on higher risk patients present an opportunity to decrease the rate of unplanned care events in patients receiving outpatient chemotherapy. Leveraging the data available in the electronic medical record to identify patients may allow for alerts to be seamlessly pushed to frontline caregivers and give them the opportunity to reach out and provide high-touch care to those in greatest need.
We are developing a predictive model for identifying patients at risk for chemotherapy-related unplanned care events during outpatient treatment as defined by the CMS OP-35 metric. This effort encompasses many aspects of data science, some of which are the following: how to clean multiple datasets each with a different structure, how to combine multiple datasets, how should the data be structured for a predictive model, how to handle missing values among the covariates, how to define the response variable, how to deal with dependencies among the covariates, how should the covariates be represented in the model, how to choose a predictive model, should the data be split into construction-validation-test sets, and how should the predictive value of the model be measured.
Anna Frackman, Resident, Anesthesiology; Sara Goldhaber-Fiebert, Clinical Professor, Anesthesiology - Effective Implementation and Use of Emergency Manuals
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
The use of cognitive aids during crises has been shown to increase appropriate care and decrease omission of vital actions across a variety of fields, including in medicine. While cognitive aids are widely used and mandated in crises in the military and aviation, adoption of these tools has been slower in medicine, and research on actual use once introduced is scarce. An emergency manual (a cognitive aid for anesthesia providers, detailing management of rare crises) was introduced to a large US hospital system in 2014. Data were collected during the first six months (period A) on whether and for what purpose an emergency manual was used in every surgical or procedural case in the hospital. Similar data were collected during a follow-up period one year later (period B), and are currently being collected at the five-year follow-up mark (period C). It is our aim to evaluate the long-term sustainability of the use of emergency manuals. The current study is specifically focusing on changes from period B to period C, as it is well known that use decreases from period A to B when even an intervention for routine use is not actively sustained. Specifically, we intend to compare overall use for each period, as well as use for rare crises.
Janice Wes Brown & Joyce Johnsrud - Incidence of Clinically Significant Human Herpesvirus 6 Infection in the Setting of Letermovir Prophylaxis after Umbilical Cord Transplantation
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigators will discuss the following project with the group. Patients are asymptomatically infected with Human Herpesvirsuses in their youth, which remain latent in the body but can later reactivate and cause potentially serious or fatal disease in immunocompromised patients. The viruses typically have intrinsic reactivation times relative to the day of allogeneic hematopoietic cell transplant (HCT) infusion but these can be influenced by various factors. We have a retrospective, single center study of 77 umbilical cord blood (UCB) transplant patients transplanted at Stanford University Medical Center (Jan 2013–Dec 2019).
Patients were grouped by initial antiviral prophylaxis (PPX), treated as Intention-to-treat. Clinically significant infection (CSI) due to Human Herpesvirus 6 (HHV-6) or Cytomegalovirus (CMV) was defined as receipt of directed antiviral therapy. With our unique population of UCB recipients who have received either valacyclovir or letermovir (LET), we would like to evaluate the impact of high-dose valacyclovir versus standard-dose acyclovir prophylaxis on the incidence of HHV6-CSI and CMV-CSI, report the incidence of HHV6-CSI and CMV-CSI with or without concomitant LET PPX, and expand our understanding of interactions between CMV and HHV-6 reactivation.
Elizabeth Lee, Senior Privacy Officer, University Privacy Office; and Andrew Brooks, Postdoctoral Fellow, Department of Genetics - How Not to be Seen
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the Data Studio Workshop will be a joint effort with our speakers, Elizabeth Lee and Andrew Brooks. Elizabeth is a Senior Privacy Officer with the Office of the Chief Risk Officer and Andrew is a Postdoctoral Fellow in Mike Snyders lab. They will discuss the topics of data privacy, re-identification risk, and shared computing for genomics, imaging, sensors, and biomedical datasets.
The HIPAA Safe Harbor Method for Deidentification does not provide the risk mitigation that research data scientists need for the long-run, especially as machine learning and natural language processing become more prevalent. During the workshop, we will consider a use case where the HIPAA Safe Harbor Method for Deidentification might not mitigate risk sufficiently. Elizabeth and Andrew will present a COVID-19 monitoring data set as an example to discuss the potential risks for its release and mitigation strategies to reduce the risk.
Given that this will be the first time we have dealt with data privacy in the workshop, we need to clarify terminology, define the problem, and set expectations. The specific strategies we will focus on during the workshop include differential computing, federated algorithms, adversarial attacks, re-identification risk rating, de-identification, and differential privacy. We expect to have multiple workshops to develop consensus around goals and ways to collaborate. The ultimate goal is to hand over to an initiative led by the University Privacy Office with participation of faculty and students who are interested in this project.
Hector Fabio Bonilla, Associate Professor, Department of Medicine, Division of Infectious Diseases - The Impact of Aripiprazole on Chronic Fatigue Syndrome
The Data Studio Workshop brings together a biomedical investigator with a group of experts for an in-depth session to solicit advice about statistical and study design issues that arise while planning or conducting a research project. This week, the investigator(s) will discuss the following project with the group.
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a chronic, debilitating illness of unknown etiology. An ME/CFS diagnosis is based solely on symptoms with case definitions made by expert consensus. According to the most recent Institute of Medicine (2015) case definition, the core symptoms of ME/CFS include debilitating fatigue, unrefreshing sleep, post-exertional malaise, and cognitive dysfunction or orthostatic intolerance. Up to 85% of patients with ME/CFS report cognitive impairment symptoms which include difficulty with memory, attention, and information processing.
Although the cause of the illness is unknown, a growing body of evidence suggests that ME/CFS involves inflammation of the brain which includes changes in inflammatory cytokines in both plasma and cerebrospinal fluid correlated with the severity of symptoms. Studies using positron emission tomography (PET) show evidence of activated microglia or astrocytes in various regions of the brain in ME/CFS patients.
Dopamine D2 receptor agonists have been shown to mediate neuroinflammation, microglial activation, and cell death in animal models and humans (4-6). This suggests that dopaminemodulating drugs may lead to clinical improvement in fatigue and cognitive symptoms in ME/CFS. Given the lack of approved drugs for treating this condition, we are interested in exploring the potential benefit of low doses of Aripiprazole.
In a retrospective study, we reviewed the medical records of 101 patients who met the criteria for an ME/CFS diagnosis according to three separate case definitions (Fukuda, CCC, and IOM) and who received off-label Aripiprazole. Medical records were included for individuals evaluated in the clinic at least twice, representing periods before and after the use of the medication. The age range was from 18 to 84 years old (mean 51 y), with a gender distribution of 67% female and 33% male, and the duration of illness was from 1 to 54 years (median 10 years). The daily oral dose of Aripiprazole ranged from 0.2-2.0 mg/day (mean 0.94 mg/day). During each clinic visit, patients were asked to rate their symptoms on a scale of 0-10.
Of the 101 patients taking Aripiprazole, 75/101 (74%) experienced an improvement in one or more categories: fatigue, brain fog, unrefreshing sleep, and frequency of post-exertional malaise (PEM) episodes. Twelve individuals (12%) had no observable difference in symptoms at the maximum dose of 2 mg, and 14 individuals (14%) reported worsening of symptoms or onset of side effects that led to discontinuation of the drug. These results suggest that Aripiprazole may effectively reduce symptoms of ME/CFS and warrants further investigation in a randomized clinical trial.
Spring 2020 Studios
Abstracts, when available, are included in the drop down
Robert Lowsky, Blood and Marrow Transplantation, & Ying Lu, Biomedical Data Science - A Novel Dose-Finding Method for a Phase 1 Clinical Trial of Kidney Graft Immune Tolerance Induction
Currently in the United States, over 100,000 patients undergoing dialysis for renal failure are on a wait list for transplantation because it offers the best chance for a near-normal lifestyle and improved life expectancy. Recipients of donor kidneys require lifelong adherence to combinations of immune suppression (IS) medications to prevent immune-mediated rejection of the graft. The unmet medical needs in solid organ transplantation are to eliminate this lifelong adherence to combinations of IS medications with their serious side effects and to prevent immune-mediated rejection. We are planning a Phase 1 clinical trial to study whether conditioning the recipient using total lymphoid irradiation (TLI), anti-thymocyte globulin (ATG), and a single very low dose of total body irradiation (svldTBI) followed by an infusion of vertebral body (VB) hematopoietic cells (HCs) will result in persistent mixed chimerism after a standard-of-care deceased donor kidney transplant. We expect that persistent mixed chimerism will result in IS drug minimization/cessation and lead to an acquired immune tolerance of the graft. One of the primary objectives is to identify the safe and effective dose of svldTBI (range 40–120 centiGray) that will support persistent mixed chimerism. We are developing a novel dose finding method that is an extension of the modified Toxicity Probability Interval design version 2 (mTPI2). This method allows escalation and de-escalation according to a pre-tabulated decision table. Our method is based on the Bayesian probability interval of toxicity and efficacy that employs a simple beta binomial hierarchical model to find the safe and effective svldTBI dose in the interval of efficacy for mixed chimerism.
Bibek Paudel, Biomedical Data Science - Spatiotemporal Modeling of Change in Healthcare Utilization due to Exposure to Wildfire Smoke
Previous studies have shown strong relation between exposure to air pollution and several health conditions, including cardiovascular and respiratory ailments. Air pollution due to wildfires have several additional complexities due to its intense and sudden nature. Therefore, as the severity and frequency of wildfires increase, understanding their effect on healthcare utilization is becoming a pressing concern. For public health officials, it is important to know how exposure to wildfire changes healthcare utilization at a population level in order to improve resource planning, preparation and decision making. We are building a predictive model that takes historical healthcare utilization and smoke exposure for individual geographical regions as inputs to predict the shortterm change in healthcare utilization.
Alexander MacInnis, MS (2017) Epidemiology, Stanford, and Lorene Nelson, Associate Professor, Epidemiology and Population Health - Cohort Case Prevalence Estimation Using Time-to-Event Analysis
Intracranial atherosclerotic disease (ICAD) is the cause of ischemic stroke in 40% of Asians, 29% of African-Americans, and 10% of Caucasians, making it the most common cause of stroke in the world. A primary goal of stroke treatment is to prevent recurrence. In cohorts with real-world standard-ofcare secondary prevention, the rate of recurrent ICAD stroke is high: over 20% of patients at 30 days from the initial stroke. The average annual rate of recurrence is 5% for all causes of stroke over the period 2000–2010. For patients with treated carotid atherosclerosis who have excellent medical and surgical options, the rate is less than 5%. This is the result of numerous major clinical trials aimed at improving secondary prevention in patients with cervical carotid atherosclerosis. In contrast, there have been only two major clinical trials for ICAD patients: WASID and SAMMPRIS. The WASID trial reported that ICAD patients with 50–99% stenosis had a 15% annual stroke recurrence with medical management. The SAMMPRIS trial included ICAD patients with 70–99% stenosis. This trial reported that treatment with aggressive medical management (including a wellness coach) was associated with a 15% annual recurrence rate compared to a 20% rate among patients who underwent an endovascular stenting procedure plus aggressive medical management. The high rates of stroke recurrence in these two trials with maximum medical management indicate that there is an urgent need for better stroke prevention regimens in this high-risk population. The same treatments that dramatically reduce the risk of stroke for patients with cervical carotid atherosclerosis do not work well enough for ICAD. We therefore need to look at new approaches for stroke prevention in ICAD patients. The most promising sources of residual risk to mitigate include thrombosis, inflammation, and lipids. We want to develop innovative clinical trials that will test promising and safe drug regimens that mitigate these sources of residual risk for secondary stroke prevention in patients with ICAD. Through these trials, we aim to make necessary progress in the fight against ICAD—the most treatment-resistant and common form of ischemic stroke in the world.
Maarten Lansberg, Neurology, Stanford University; Kevin Sheth, Neurology, Yale University; and Adam de Havenon, Neurology, University of Utah - Innovative Trial Design for Secondary Stroke Prevention
In December 2019, a series of pneumonia cases emerged in Wuhan, Hubei, China. Sequencing subsequently identified a novel coronavirus, which was named COVID-19. On March 11th 2020, the World Health Organization declared a pandemic and as of April 18th 2020, approximately 2.5 million people have been infected and at least 158,000 have died. The primary driver of COVID-19 morbidity and mortality is respiratory compromise. This is thought to be linked with increases of certain elements of the extracellular matrix, one of which is a matrix polymer known to drive inflammation in multiple other tissues and disease models. We are planning a proof-of-concept study to evaluate the clinical utility of a repurposed agent that inhibits the synthesis of an extracellular matrix polymer which may be a means of managing the respiratory morbidity of COVID-19 infection. The repurposed agent was developed in the 1970s and approved in Europe. However, it has been neither reviewed nor approved by the FDA. If successful, this may prove to be a low cost and easily adhered to medication with significant benefit in both the USA and the developing world. For the study design, we are considering an international, multi-center, 3-week, 2:1 randomized, phase 1/2 study of this repurposed agent as treatment versus standard of care with at most 40–45 subjects. One of the primary objectives is to identify the safe and effective dose. Other endpoints, that will be looked on in a largely exploratory manner, will include the ability of the repurposed agent to improve time to worsening in oxygenation requirement, time to mechanical ventilation, duration of hospital stay, and mortality.
Andrew Wardle, Visiting Scholar, Immunology, and Paul Bollyky, Associate Professor, Infectious Disease and Immunology - Design for the INHALE Clinical Trial: Avoidance of Lung Events in COVID-19
In December 2019, a series of pneumonia cases emerged in Wuhan, Hubei, China. Sequencing subsequently identified a novel coronavirus, which was named COVID-19. On March 11th 2020, the World Health Organization declared a pandemic and as of April 18th 2020, approximately 2.5 million people have been infected and at least 158,000 have died. The primary driver of COVID-19 morbidity and mortality is respiratory compromise. This is thought to be linked with increases of certain elements of the extracellular matrix, one of which is a matrix polymer known to drive inflammation in multiple other tissues and disease models. We are planning a proof-of-concept study to evaluate the clinical utility of a repurposed agent that inhibits the synthesis of an extracellular matrix polymer which may be a means of managing the respiratory morbidity of COVID-19 infection. The repurposed agent was developed in the 1970s and approved in Europe. However, it has been neither reviewed nor approved by the FDA. If successful, this may prove to be a low cost and easily adhered to medication with significant benefit in both the USA and the developing world. For the study design, we are considering an international, multi-center, 3-week, 2:1 randomized, phase 1/2 study of this repurposed agent as treatment versus standard of care with at most 40–45 subjects. One of the primary objectives is to identify the safe and effective dose. Other endpoints, that will be looked on in a largely exploratory manner, will include the ability of the repurposed agent to improve time to worsening in oxygenation requirement, time to mechanical ventilation, duration of hospital stay, and mortality.
Angela Lumba-Brown, Pediatric Emergency Medicine - Recovery Course in Children with Complicated Mild Traumatic Brain Injury
More than 260,000 US emergency department visits for pediatric mild traumatic brain injury (mild TBI) each year are complicated by intracranial bleeding that is often undiagnosed or sparsely monitored after hospital discharge. Mild TBI is defined as a head injury resulting in a Glasgow Coma Scale score of 13 or higher in a child with amnesia, transient neurologic symptoms, and/or brief loss of consciousness. National guidelines and preliminary research suggest that children with intracranial bleeding in the setting of mild TBI, commonly referred to as complicated mild TBI, may be at risk for prolonged recovery and future disability. One-third of all children with mild TBI have prolonged symptom-recovery beyond one month that impacts their families, reintegration to school and learning, and quality of life. However, the proportion of children with prolonged recovery secondary specifically to complicated mild TBI is unknown. Children with and without complicated mild TBI are currently managed almost identically and therefore, there is a critical need to understand differences in their outcomes. Without such information, informing the need for diagnostic neuroimaging and quantifying the benefits of management with early therapeutic intervention in this population remains unknown. This study’s overall objectives are to: 1) test if children with complicated mild TBI have longer recovery times when compared to those without complicated mild TBI and 2) test if children with complicated mild TBI at one year post-injury have a higher proportion of academic difficulty and lower quality of life when compared with those without complicated mild TBI. My central hypothesis, supported by preliminary data, is that children with complicated mild TBI have longer recovery times and higher risk for future academic difficulties at one year post-injury as compared to children without complicated mild TBI.
Lihua Lei, Postdoctoral Fellow, Statistics; Emmanuel Candès, Professor, Statistics; and Chiara Sabatti, Professor, Biomedical Data Science - Survival Analysis of COVID-19 Patients
The COVID-19 pandemic has placed extraordinary demands on health systems. These unprecedented demands create the urgent need for medical resource allocation. Our goal is to build a transparent data-driven system that will assist decision making for front-line workers. The first step of our project is to build a patient-level risk assessment tool based on survival analysis. We integrated over 15 publicly available data sources and performed extensive data cleaning, de-duplication, and filtering to build a database for more than 10 countries and regions in the world. For each subgroup, we performed elementary survival analyses and presented our results on a website (https://zren.shinyapps.io/covid19/). The main challenge we are facing is to handle the missing values (e.g. age and gender) in those publicly available datasets that are unlikely to be missing at random. We therefore use the population statistics and apply inverse probability weighting techniques to adjust for the non-random missing values under some assumptions about the missingness mechanism. We further propose a method without those assumptions based on partial identification, although it is conservative and computationally intensive.
Michael B. Sklar, Statistics; Philip W. Lavori, Biomedical Data Science - A Contextual Multi-Arm Bandit for Surgical Treatment of Lumbar Stenosis
The VA SOLID study will test the utility of a Contextual Multi-Arm Bandit (CMAB) design for improving patient outcomes in the surgical treatment of spinal stenosis across multiple VA systems. Surgical treatment of spinal stenosis is broadly described as decompression of trapped neural components) alone or in conjunction with spinal fusion (to stabilize the spine). While decompression alone is associated with lower morbidity and cost, both failure to relieve symptoms and the possibility of post-operative spinal instability encourage the addition of spinal fusion. The Stanford statistical advisory group is responsible for proposing a specific method for outcomedependent, contextual adaptation of randomized assignment of treatment in order to (1) improve within-sample average patient outcome and (2) generate reliable decision rules (based on patient context) for future treatment decisions. As a first step, Michael Sklar has completed a review of technical publications that might inform design of a CMAB for medical/surgical decision-making, and begun work on simulations of the performance of the leading contenders.
Alice Bertaina, Stem Cell Transplantation and Regenerative Medicine - Innovative Trial Design for T-allo10 Cell Infusion after αβhaplo-HSCT
Acute leukemia is the most common cancer in children and teens, accounting for almost 1 out of 3 cancers. Despite recent advances in the treatment of childhood leukemia, a substantial proportion of patients are resistant to conventional treatment. Allogeneic hematopoietic stem cell transplantation (HSCT) is effective for high risk or refractory disease but is limited by a lack of HLA-matched donors. Haploidentical HSCT after αβT-cell/CD19 B-cell depletion (αβhaplo-HSCT) can address this issue. It is especially valuable for patients of African-American or mixed heritage because this demographic has a significantly lower likelihood of finding a matched donor. αβhaplo-HSCT has extremely low rates of transplant-related mortality (TRM) and severe graft-versus-host disease (GvHD). However, the rate of leukemic relapse (25–30%) after αβhaplo-HSCT remains high. Thus, there is a clinical need to improve the anti-leukemic efficacy of αβhaplo-HSCT without increasing the risk of GvHD. We are planning a Phase I/II clinical trial combining αβhaplo-HSCT with T-allo10 cell infusion. The donor cells in the T-allo10 infusion are processed to strengthen immunosuppression thereby decreasing the risk of GvHD and to promote graft-versus-leukemia (GvL) activity. The primary objective of the Phase I part is to identify the safe and effective dose of T-allo10 cells (range 1 ×105 to 1×106 cells/kg recipient body weight) which can be infused in patients without increasing risk of GvHD. The primary objective of the Phase II part is to evaluate the improvement of the adaptive immune reconstitution defined as an increase of absolute CD4 cell count at Day 100 compared with historical controls.
Winter 2020 Studios
Abstracts, when available, are included in the drop down
Professor Michael Eisenberg (Department of Urology, Stanford University) & Maarten Wensink (Department of Epidemiology, Biostatistics, and Biodemography, University of Southern Denmark) - Association between Paternal Medication Use Prior to Conception and Adverse Birth Outcomes
Congenital birth defects affect 3% of births in the United States. Several parental factors, such as smoking and increasing age, been shown to modify the incidence. Given the longer and more obvious influence a mother has on gestation, most risk factors for birth defects have focused on women. However, as the age of paternity at conception increases around the developed world, paternal comorbidities increase. With that, more prospective fathers are exposed to prescription medications during spermatogenesis cycles, which lead to live births. Our ability to adequately counsel patients regarding paternal exposures to medicines is limited by sparse data. Investigators have performed studies on limited numbers of patients exposed to certain medications strongly suspected of impacting sperm DNA (e.g. anti-neoplastics). Some common medications, such as antidepressants, may affect the DNA integrity of sperm. To date, large studies of diverse medications are rare despite the crucial role the sperm contributes to fertilization and the first few days of development. This project explores the association between paternal medication use and adverse birth outcomes, including congenital birth defects. Using unique national identification numbers, we will link Danish demographic, birth, health, and medication registries for the approximately 1.3 million births from 1995 to 2015. Next, we will determine if individual medications or classes of medications with known spermatogenic effects taken by fathers just before conception are associated with a higher risk of congenital birth defects. Such findings are likely to have wide implications for couples attempting to conceive and provide guidance for the safety of medications during reproductive efforts.
James Zou (Department of Biomedical Data Science) & Ruishan Liu (Department of Electrical Engineering) - Eligibility Criteria Relaxation and Optimization for Clinical Trials
Clinical trials use strict eligibility criteria to exclude patients who may have poor outcomes. Those criteria are designed based on physician’s expectation and are usually duplicated across protocols without solid clinical validation. Unnecessarily stringent criteria have been a large barrier in trial accrual—the enrollment is significantly slowed down and the generalizability of results is limited. Relaxing the eligibility criteria has been a popular advocate but how to really do it remains underexplored. In this work, we emulate oncology cancer trials from observational data and systematically analyze how different eligibility criteria can affect a trial’s final performance. Our results validate the necessity to broaden overly restrictive enrollment because patients excluded by the original criteria often derive similar clinical benefits as the enrolled ones. We propose a principled framework to encode different eligibility criteria and emulate corresponding trials. Given standard inclusion and exclusion criteria, we are able to evaluate the influence of each criterion and recommend an optimal strategy to relax them. It is a powerful tool to identify potential label expansions for existing trials and facilitate the design of eligibility criteria for future trials. It can also be used to generate synthetic external control arms with its unified pipeline to conduct cohort selection on observational data.
Bruce Ling (Pediatric Surgery) & Shiying Hao (Pediatric Cardiac Surgery) - Early Detection of Preeclampsia
Preeclampsia (PE), a pregnancy-related placental vascular disorder affecting 5–8% of all pregnancies, is thought to be a multisystem disorder of pregnancy driven by alterations in placental function and resolved by the delivery of the placenta and fetus. Untreated PE can cause serious health problems for both mothers and babies. Early detection of risk of developing PE remains a challenge in clinical settings. The ratio of soluble fms-like tyrosine kinase (sFlt-1) and placental growth factor (PIGF) levels has been proposed as a useful index to diagnose and manage PE. However, the ratio only works at mid or late gestation. Previous transcriptomic and proteomic profiling of normal and complicated pregnancies have identified disease-specific expression patterns and signaling networks, which suggests candidate biomarkers for possible early clinical assessment. We hypothesized that there are maternal serological biomarkers differentiating impending PE from normal pregnancy at early stage of gestation. We quantified proteins and lipids in maternal serum by ELISA and LC MS/MS methods, and evaluated the performance of these candidate markers in predicting PE on an age-matched discovery cohort (32 PE subjects and 32 controls) and a longitudinal testing cohort (20 PE subjects and 20 controls). Results showed that a ratio of an elevated marker and a decreased marker differentiated women with impending PE from normal pregnant women at 1st and early 2nd trimesters, which is earlier than the well-established biomarkers (sFlt-1 and PlGF). Our finding may offer a new investigational approach towards the understanding of biology during pregnancy as well as guiding innovative methods for PE assessment.
Guangbo Chen (Institute for Immunity, Transplantation, and Infection) - Early Detection of Skin and Other Cancers
Each year in the United States, 1.8 million new patients are diagnosed with cancers. Beyond this coverage by the NCI SEER registry, 3.3 million additional new patients are diagnosed with nonmelanoma skin cancers in US annually. Even a moderate improvement in earlier detection (e.g., 6 months) could have meaningful benefits for survival and costs. The cancer development has been intensively investigated using samples collected after diagnosis. However, cancer development prior to clinical presentation remains mostly unobserved due to scarcity of samples. At Stanford, we have created a prospective longitudinal cohort of individuals followed for up to 10 years. Immune profiling of these individuals is systematically characterized through annual visits. During the period of observation, 48 incidences of malignancies were recorded (67% of them were non-melanoma skin cancers, consistent with the overall US population). Thus, the immune profiling of blood samples collected prior to the cancer diagnosis offers a rare opportunity to understand changes in the immune system during this crucial period.
In these samples, we found that the average concentrations of Cancer-Preceding (CanDx) cytokines were already elevated up to 3 years before the clinical diagnosis. Even at this time point, the impact of cancers on the immune system is large. It is comparable or more significant than the impact associated with over 50 years of aging. We also observed that average concentration of CanDx cytokines decreased immediately in the years following the cancer diagnosis. This is consistent with the fact that most of the incidences of cancers in our cohort, as well as the general US population, were basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). These are nearly always surgically removed soon after diagnosis. Lastly, we also found evidence suggesting that a tilted inflammation balance in aged population may contribute to accelerated cancer development.
Our current dataset is not powered for detailed analyses on cancer subtypes other than nonmelanoma skin cancers (BCC/SCC). We are expanding our current study cohort by both active recruitments targeting cancer-prone populations and large-scale electronic health record analyses. Our aim is to examine the role of immunity in early cancer development beyond skin cancers.
Yan Min (Epidemiology and Population Health) - Metabolite-mediated Sex-specific Associations between Microbiome and Fat Distribution
We hypothesize that there are different sex-specific microbial signatures linked to regional adiposity in men and women. Such differences could be largely attributable to the biological functions of sex hormones and fatty acids. Sex hormones have been shown to be associated with both regional adiposity and gut microbiota. Fatty acids from the lipid pathways have shown pronounced effect in the mechanism of determining the adiposity site, whereas amino acids were shown to play catalyst roles in this process. To examine the above hypothesis, our current study has two aims. First, identify the sex-specific microbial compositions that associate with fat distribution in men and women. Second, identify the metabolites that could be potential mediators to the association between the microbial signature and fat distribution. To achieve these two aims, we conducted the following analyses separately in women and men. First, we univariately screened the metabolites that are associated with fat distribution by sex. Second, we explored the sex-specific microbial signatures using the Wald test. Third, we implemented sparse partial least square discriminant analysis to synthesize the joint distribution across microbiome, metabolites, and fat distribution. Fourth, we conducted mediation analysis to identify the metabolic mediators for the association between microbiome and fat distribution.
Rusty Hofmann (Professor and Chief, Interventional Radiology) - Causal Effect Estimation of First-Line Treatments on Survival for Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC) is a common and aggressive form of liver cancer that results in 800,000 deaths globally each year. In the US, HCC accounts for the fastest-rising cause of cancer mortality. While various treatment options are available for HCC ranging from different types of surgeries (e.g. liver transplant, chemoembolization, resection, ablation) to different types of chemotherapies (e.g. systemic chemotherapy, chemotherapy infusion), selection of patient-specific treatment options for HCC remains challenging.
As an initial attempt to investigate this question, we study a cross-sectional dataset of 2,625 HCC patients derived from the Stanford University Medical Center. We estimate the conditional average treatment effect (CATE) using causal random forests on a subset of 206 patients that received systemic chemotherapy as first-line treatment (controlled group) versus another subset of 953 patients that received chemoembolization as first-line treatment (treatment group). We adjusted for covariates including demographics, TNM staging covariates, lab test values, and liver disease history. We observe a CATE of 13.0% ± 4.0% absolute difference in the three-year survival probability between the treatment group and the controlled group.
Robert M. Waymouth (Department of Chemistry) - Charge-altering releasable transporters (CARTs): dynamic materials for delivery and release of mRNA
Our team has recently discovered a general, safe, and remarkably effective concept for RNA delivery based on a new class of synthetic cationic materials, Charge-Altering Releasable Transporters (CARTs). These new materials operate by an unprecedented mechanism for the delivery and transcription of proteins in both cell culture and live animals. The function and selectivity of these materials has proven to be remarkably sensitive to aspects of the chemical structure, leading to (for instance) in vivo selective accumulation changing from spleen (> 99%) to lung (75%) upon changes in chemical structure. Due to the modular design of these materials and our ability to rapidly synthesize new candidates, there is a vast chemical space to explore. Our hope is to apply statistical design of experiment (DoE) methods to explore this space efficiently and establish meaningful structure-function correlations to guide our understanding of the remarkable efficacy of these materials. Further convoluting the possible space to explore, we have found that mixing chemically different CARTs in a single transfection often leads to superior function over either component individually, sometimes dramatically superior.
Fall 2019 Studios
Abstracts, when available, are included in the drop down
Pamela Flood, Professor of Anesthesiology, Perioperative and Pain Medicine (OB); and Haley Hedlin, Biostatistician, Quantitative Sciences Unit - Prevention of Persistent Opioid use in Mothers
Opioid-sparing analgesic strategies are desperately needed for pregnant women at risk for prolonged pain and opioid use after surgical delivery. This is the largest iatrogenic exposure of young women to opioids in the United States. Each year, approximately 1.2 million American women undergo the most common surgical procedure. Up to 11% will persist with analgesic use, reporting prolonged pain and reduced function.
I propose a double-blind, randomized clinical trial of gabapentin which is titrated over 12 weeks compared to placebo. The primary outcome is time to opioid cessation. Secondary outcomes are pain resolution, return of physical function, and psychological wellbeing. I have enrolled over 30 subjects with 2 lost to follow-up before achieving the primary outcome variable of time to opioid cessation.
My need for statistical advice concerns the statistical analysis plan and the sample size calculation. The study is designed with a time to event outcome. In my current plan, event times are measured every 2 weeks. However, most of the events occur in the 26 week range. I also have count data measured at each of the 2-week measurements but need help to incorporate these into the study design. The patient population is relatively limited. Therefore, I need help finding an appropriate design that will be sufficiently powered.
Laurel Crosby, Research Engineer, Stanford Genome Technology Center - Impact of Organic Mercury Exposure on Selenium Bioavailability in Chronic Fatigue Syndrome
Organic forms of mercury (Hg) are ubiquitous contaminants in fish, but the toxic health effects of mercury are mitigated by binding with the essential trace metal selenium. Selenium (Se) is also a required cofactor for enzymes that manage oxidative stress and for thyroid hormone metabolism. However, functional deficiency in these enzymes may not be apparent by measuring selenium concentrations or using comprehensive thyroid hormone assessment panels. Chronic Fatigue Syndrome, also known as Myalgic Encephalomyelitis (ME/CFS), is a complex multi-system disorder that is characterized by increased levels of oxidative stress, neuroinflammation, disturbances in energy metabolism, and other nonspecific markers of illness. We have identified a subset of ME/CFS patients with elevated levels of mercury in hair and a molar ratio of Se:Hg less than 1, possibly indicating lowered bioavailability of selenium in vivo. Our findings may explain the recent report of a Low Free T3 Syndrome in a subset of ME/CFS patients, as free T3 levels are dependent on selenium for thyroxine (T4) deiodinase activity.
We need help with the study design and statistical analyses needed to address the following scientific questions.
1. ME/CFS patients
(a) Does the Se:Hg ratio correlate with selenoenzyme activity?
(b) Does selenoenzyme activity correlate with phenotypes defined by two different diagnostic standards?
2. Non-ME/CFS controls
(a) Does the Se:Hg ratio correlate with selenoenzyme activity?
3. Is there a way to tease apart the causal direction between diet and a subgroup of ME/CFS patients?
Alice Fan, Assistant Professor, Medicine-Oncology; and Christian Hoerner, Research Scientist, Canary Center at Stanford for Cancer Early Detection - Platelet Transcriptome for Early Detection of Kidney Cancer
In renal cell carcinoma (RCC), the 7th most commonly diagnosed cancer in the U.S., time of diagnosis has a profound impact on survival. For stage I patients (localized non-invading tumor < 7 cm), the 5-year overall survival rate is 96%, compared to 23% for stage IV (metastatic) patients. There are currently no screening assays for RCC, hence it is often found incidentally and ˜30–40% of patients are still diagnosed with poor-prognosis, advanced (stage III or IV) RCC, which highlights the need for early detection and practical screening assays.
Once a small renal mass has been found by imaging, the treatment decision for surgery versus surveillance is made based on tumor features (histologic subtype, growth rate, tumor grade, which is a measure of tumor aggressiveness) and condition of the patient (age, comorbidities). However, information on tumor grade cannot be readily obtained through imaging or tumor biopsies, hence there is a need for a surrogate marker for tumor grade to aid in diagnosis and clinical management of small renal masses.
Platelets splice pre-mRNA deposited by megakaryocytes, which is the bone marrow cell type from which platelets are derived, splice it into mature mRNA, and translate it into protein. While the platelet transcriptome is remarkably stable over time in healthy individuals, platelets have been shown to respond to various disease states, including cardiovascular and autoimmune disease, and more recently, cancer, with likely disease-specific changes in the platelet transcriptome. However, platelet transcriptomic changes have never been specifically investigated in RCC or in early stage cancer or in high-grade tumors.
Jessica Ansari, Clinical Assistant Professor, Department of Anesthesiology, Perioperative and Pain Medicine - Calcium Chloride in the Prevention of Uterine Atony during Cesarean
Maternal hemorrhage is globally the leading cause of maternal mortality. Furthermore, 80% of postpartum hemorrhage is caused by uterine atony which is a failure of the uterus to contract after separation of the placenta. Current drugs used to address uterine atony refractory to standard management with oxytocin are limited by cost, adverse side effect profiles, and common contraindications such as hypertension and asthma.
Calcium chloride is a widely-available, shelf-stable, cheap, and well-tolerated drug. Calcium is a key element in uterine muscle contractility. The mechanism of action for all drugs currently used for uterine atony depends upon myometrial calcium. Multiple studies utilizing uterine muscle strips from pregnant animals and humans have shown that increased extracellular calcium can improve strength and frequency of uterine contractions. Finally, many experienced obstetric anesthesiologists anecdotally use calcium to address cases of refractory uterine atony. However, there are no clinical studies that have examined the role of calcium chloride in this setting.
This pilot study is aimed to elucidate the potential role of calcium chloride plus standard of care for prevention of uterine atony in women at high risk undergoing Cesarean section. The design of this interventional pilot clinical trial is safety and efficacy with double-blind masking and parallel assignment via randomized allocation to either treatment or placebo for the purpose of prevention of uterine atony. A total of 40 parturients undergoing Cesarean with 2 or more accepted risk factors for uterine atony were block-randomized in a one-to-one ratio to receive an intravenous infusion of either calcium chloride or placebo at the time of fetal delivery. The primary aim is to determine if a single dose of calcium chloride compared to placebo administered immediately after fetal delivery can reduce the incidence of uterine atony in women at risk. The secondary aims are to determine whether intravenous calcium chloride reduces blood loss, improves maternal hemodynamics, and is well-tolerated with a favorable side-effect profile. The primary outcome is dichotomous: presence or absence of clinical uterine atony. The secondary outcomes include quantitative blood loss, subjective assessment of uterine tone from 0% (no tone) to 100% (excellent tone) by the obstetrician immediately after completion of study drug infusion, and change in hematocrit defined as preoperative baseline minus postpartum day 1
FIRST SESSION INVESTIGATOR: Qian Zhao, Doctoral Candidate, Department of Statistics, and SECOND SESSION INVESTIGATOR: Valerie Chock, Associate Professor of Neonatology, Department of Pediatrics - FIRST SESSION: Forecasting Platelet Demand to Reduce Inventory Wastage, SECOND: Cerebral Oxygenation and Autoregulation in Preterm Infants
FIRST SESSION:
Platelets are the blood component responsible for clot formation. The greatest demand for this blood product comes from trauma, oncology, and major surgery patients. Hospitals must always maintain a sufficient inventory of platelets. Platelets have a shelf life of only five days but spend two in testing for bacterial and viral contamination. This means that hospitals have only three days to use platelets upon receiving them. This constraint, along with highly variable demand, a smaller donor pool, longer donation process, and less collection capacity due to the cost of specialized equipment, makes platelets the most difficult blood product for hospitals to manage. It is estimated that nationwide, 11% of all collected platelet units, or 250,000 units, expire before being transfused, amounting to $80 million lost and 500,000 donor-hours wasted. In 2017, the Stanford Blood Center sought to address this wastage problem by engaging a team of researchers to forecast platelet demand using daily aggregated hospital data. They formulated a three-day ordering strategy by solving an optimization problem using features aggregated from the available data. However, the ordering strategy was not put into production due to lack of trust in model predictions by the inventory manager. In order to address this problem, we decided to separately predict platelet demand, and develop ordering strategy as a secondary step. The goal of our current study is to supply the user with a decision support tool which will build confidence in the accuracy of computer predictions. Our four-day daily prediction is based on both aggregate data and patient-level information. Our questions concern how to improve the prediction models.
SECOND SESSION:
Improved understanding of the relationship between altered hemodynamics and cerebral oxygenation may inform future strategies to prevent brain injury in preterm infants. The objective of this study is to determine whether decreased cerebral oxygenation or altered cerebral autoregulation in the first 96 hours of life is associated with mortality or severe neuroradiographic abnormalities in preterm infants. The study design is a prospective cohort over multiple centers. We enrolled 111 preterm infants from 6 neonatal intensive care units. These preterm infants had birth weight less than 1250 g during the first 24 hours of life and received simultaneous monitoring of mean arterial blood pressure and cerebral oxygenation using near-infrared spectroscopy until at least 96 hours of age. The primary outcome measure is mortality before hospital discharge or severe neuroradiographic abnormalities. Among the enrolled preterm infants, 103 had sufficient spectroscopic data for analysis. We computed positive or negative moving window correlations between cerebral oxygen saturation (Csat) and mean arterial blood pressure (MAP) to determine time periods with altered cerebral autoregulation. We compared percentage of time with altered autoregulation using Spearman rank correlation between infants with and without adverse outcome. We have specific questions about how to analyze the longitudinal data collected from these preterm infants.
Angela Lumba-Brown, Clinical Assistant Professor, Departments of Emergency Medicine and Pediatrics - Subtype-based Early Intervention in Pediatric Concussion
Concussion affects millions of children in the United States each year with recovery times averaging 4 weeks, subsequently impacting quality of life. Current acute concussion care is solely supportive care with a gradual return to activity and is not based on newer concussion subtype management. While a proportion of children with head injury present to the pediatric emergency department (ED), these often represent the most severe presentations representing the most ideal therapeutic target.
We hypothesize that children diagnosed in the pediatric ED can be feasibly classified into concussion subtypes and directed to acute subtype-based targeted therapies with shorter recovery times as compared to those who receive standard of care. We propose an observational study on epidemiology followed by a cross-sectional trial for interventional feasibility. Our questions concern study design and data analysis methods.
Wei Jiang, Instructor, Division of Human Gene Therapy, Department of Pediatrics - The Role of T-cells in the Autoimmune Etiology of Narcolepsy
Individuals with narcolepsy suffer from abnormal sleep patterns due to loss of neurons that uniquely supply hypocretin (HCRT), a wakefulness-promoting hormone in human brains. Previous studies found the associations of narcolepsy with human leukocyte antigen (HLA)-DQ6 allele and T-cell-receptor-alpha (TRA) J24 gene segment. These led to an autoimmune hypothesis for narcolepsy that the presentation of HCRT-derived peptides by DQ6-expressing antigen presenting cells to TRAJ24-expressing T-cells drives T-cell clonal expansion and downstream self-attacking immune responses against HCRT-producing neurons. Although T-cells from narcolepsy patients were recently reported to recognize HCRT peptides, autoimmunity-related evidence that HCRT-reactive T-cells have experienced in vivo clonal expansion is still absent.
We directly sequence T-cell-receptor (TCR) and selected phenotypic marker genes in over 5000 single ex vivo T-cells that are isolated from DQ6+ donors using DQ6-HCRT peptide tetramers. Statistical comparisons suggest that DQ6-HCRT(87–100) tetramers, a peptide composed of amino acids 87–97 from HCRT, identify significantly more expanded CD4+ T cells from 8 patients than from 8 DQ6 allele-matched healthy controls. We also identify related TRAJ24+ TCR clonotypes encoded by identical genes from 2 patients and 2 controls. TRAJ24-G-allele+ clonotypes only expand in the two patients, whereas a TRAJ24-C-allele+ clonotype expands in a control (the G/C SNP in TRAJ24 gene is narcolepsy-associated). In addition, clonally expanded TRAJ24-G-allele+ T-cells from the two patients exhibit an unconventional effector phenotype. Our identification of features distinguishing in vivo expansion of HCRT-specific TRAJ24+ T-cells in pat.
Spring 2019 Studios
Abstracts, when available, are included in the drop down
Jane Kim, Clinical Assistant Professor, Psychiatry & Behavioral Sciences at Stanford - Ethical considerations in online bandit problems and offline policy evaluation in mHealth
I am planning a career development grant on the topic of incorporating ethical principles in the design and analysis of online learning algorithms used for mobile health apps, e.g.contextual bandits. The overall goal is to articulate and identify considerations that may be needed to ensure that online learning algorithms can be deployed in an ethically robust mannerthat is in alignment with the Belmont principles. My goal for the session is to brainstorm to see what ideas people have about incorporating ethical principles into the design or analysis of bandits, and how to narrow the scope of potential ideas.
Vivian Saper, Pediatrics, Division of Human Gene Therapy - Series Two: sJIA and lung disease
In association with a treatment shift to new biologic drugs inhibiting cytokines IL-1 and IL-6, a portion of children with systemic onset juvenile idiopathic arthritis (sJIA) have been developing an unusual and often fatal lung disease. Initial characterization has been accomplished by Dr. Saper and colleagues in the first international series of 61 cases. Over 50 further cases have been identified allowing an opportunity to focus on the issues of disease severity prior to the lung complication and on drug association. For this next project, Dr. Saper would like an analytic plan to best direct data capture in the next REDCap-based survey which is preliminarily built. Control cases are imperfectly available and this needs to be addressed as best as possible.
Laurel Stell, Research Engineer, Stanford Biomedical Data Science - An Introduction to ggplot2 for Advanced Graphics in R
Still using base graphics in R? Struggling to visualize your data in a way that reveals its secrets? Would you like your plots to look more professional? Tired of using clunky tools (such as par() and for() loops) to arrange multiple plots in one figure? This presentation will help you get started using ggplot2 and on the path to more beautiful and informative visualizations with less code and frustration. I will provide many examples, tips for learning more, and the R Markdown file used to create the slides.
Access Slides and RMD file.
Suzann Pershing, Ophthalmology, & Tina Hernandez-Boussard, Medicine - Biomedical Informatics - Leveraging Big Data to Assess the Impact of Vision and Eye Surgery on Dementia
Preliminary data have suggested improved cognitive outcomes among dementia patients who underwent cataract surgery but that patients with dementia are only half as likely to undergo cataract surgery compared to those without dementia. We are writing a proposal to use longitudinal VA EHR data to 1) develop a database with electronic phenotypes for dementia and visual impairment and 2) evaluate the impact of cataract surgery on dementia incidence and progression. In this Data Studio consultation, we would like to discuss 1) how to model impact of cataract surgery on dementia incidence and 2) how to model dementia progression as a function of time after cataract surgery.
Roham Zamanian, Medicine - Pulmonary & Critical Care Medicine - Master protocols in pulmonary arterial hypertension (PAH)
Winter 2019 Studios
Abstracts, when available, are included in the drop down
Liang Liang, Postdoctoral Fellow in Genetics at Stanford - Longitudinal profiling of biomarkers in human pregnancy
This project is studying the natural trajectory of various biomarkers during pregnancy. The ultimate goal is to choose a panel of selected biomarkers that can be monitored in order to identify women with higher risk of miscarriage or premature delivery.
Justine Maller, Postdoctoral Medical Fellow in Pediatric Rheumatology at Stanford - Extracellular vesicles in systemic juvenile idiopathic arthritis: clues to pathogenesis and biomarkers of disease
This research is focused on studying systemic juvenile idiopathic arthritis (sJIA), a pediatric autoinflammatory disease of unknown etiology. Diagnosis can often be challenging, and not all patients with sJIA respond optimally to biologic cytokine inhibitors, highlighting two of the many unmet needs in understanding and treating this disease. I am working with plasma samples and implementing high-resolution flow cytometry to characterize the differences in extracellular vesicle (EV) populations (based on surface marker expression) present in active relative to quiescent disease states as well as compared to healthy controls. The overall objective of this study aims to identify EV signatures that distinguish active and quiescent states of sJIA, which could reveal novel biomarkers with exciting diagnostic, prognostic, and therapeutic potential.
Elliott Main, Clinical Professor in Obstetrics & Gynecology at Stanford - Adjusting for risk factors when comparing cesarean birth rates between hospitals
The Nulliparous, Term, Singleton, Vertex (NTSV) Cesarean Birth Rate measures the proportion of cesarean births among a population of women deemed to be at very low risk of needing a cesarean section (CS). Distributions of many of the risk factors (such as obesity, age and gestational diabetes) may still differ significantly between providers and the adjustment may result in different comparison results. The outstanding question is whether those factors should be taken into account when comparing CS rates between hospitals. If so, what is the most appropriate statistical method for adjustment?
Laura Hack, Clinical Instructor in Psychiatry and Behavioral Sciences at Stanford - Biotype-guided (BiG) treatment trial for major depressive disorder: using neuroimaging markers to personalize antidepressant therapy
The Williams PanLab is designing the first prospective trial of depression using brain activity from fMRI in particular regions to guide subjects to treatment. We are inspired by innovative clinical trial designs used in cancer medicine but have questions about the most appropriate design and statistical approaches given the nature of our data and the questions we are trying to answer.
Laurel Stell, Research Associate in Biomedical Data Science at Stanford - Accounting for unobserved factors when testing RNA seq data for differential expression
Unobserved technical and biological factors can affect RNA-seq data, resulting in both false positives and loss of power when testing for differential expression between groups. This problem is widespread and commonly handled with surrogate variable analysis (SVA), using the sva or SmartSVA package in R to estimate the number of latent factors as well as the factors themselves. Unfortunately, these algorithms may fail under some conditions such as strong correlations between the factors and the variable being tested for differential expression. Newer packages such as cate address these issues. I will discuss both theory and practical implications and give examples from real world data. I will make the slides and sample code publicly available, although the data cannot yet be released. For slides and R code, click here.
Mark Hlatky (Professor of Health Research and Policy at Stanford) & Marc Søndergaard (Graduate of Health Research and Policy at Stanford) - I wish we’d measured that at the start! Filling in missing baseline data based on a (biased) sample
We are interested in the question of whether adverse pregnancy outcomes (APOs) in women, like gestational diabetes, are risk factors for developing heart disease in later life. We are working with the Women’s Health Initiative (WHI) data for the study. This is a large cohort of women (about 161,000) enrolled about 20 years ago, with extensive baseline data collection and scrupulous follow-up for detecting the development of heart disease. So the cohort is ideal for our study, BUT the investigators didn’t collect baseline data on APOs, the exposure of interest. So we did a survey in 2017 to collect data on APOs from about 51,000 women, and are trying to devise the best analysis strategy to relate APOs to heart disease. Our “missing data problems” range from small (some of the 50,000 respondents did not answer all the survey questions, but did answer some of them) to very large (we are missing baseline APO data on about 110,000 women, many of whom have died from heart disease or other causes).
Fall 2018 Studios
Abstracts, when available, are included in the drop down
Balasubramanian Narasimhan (Stanford Biomedical Data Science) and Neal Birkett (Cancer Clinical Trials Office) - Automatic generation of clinical trial reports
This will be an interactive session between the members of Cancer Clinical Trials Office (CCTO) at Stanford and Department of Biomedical Data Science (DBDS) to explore processes that might expedite NIH reporting for clinical trials. Neal Birkett from CCTO will speak about reporting workflow in use and present some examples. Balasubramanian Narasimhan from DBDS will talk about some R based tools that may be useful in this context using a recent report he created as example. Time permitting, we will discuss the possibility of piloting some reporting templates and associated issues.
Kari Nadeau (Stanford Medicine & Pediatrics) - Adaptive clinical trial design for milk allergy trial
The integrative, precision health-based science and inter-departmental collaborations fostered at the Stanford School of Medicine have created transformative change in preventing and predicting allergic and asthma disorders.The Sean N. Parker Center for Allergy and Asthma Research focuses on finding the cause and cure of allergies and asthma. The center has been very successful in basic and clinical research, including 20 clinical trials in 2018, most in phase 1 and 2 but some of phase 3 studies. We have worked with biostatisticians from QSU.
Recent medical discoveries in allergic and asthma disorders are similar to oncology that we have more precise disease types and multiple drugs are being developed. We are interested in using precision approaches, such as basket trials, platform trials, and master protocols to accelerate our clinical trial research. We plan to discuss a phase 2 trial on managing gastrointestinal adverse events in patients undergoing milk protein oral immunotherapy. We would seek inputs on design features to maximize the utility of this planned phase 2 trial. Background information on this particular trial and related clinical trial challenges in allergic and asthma disorders in general can be found from the following literature.
Jorg Goronzy & Chulwoo Kim (Stanford Immunology and Rheumatology) - Estimating the number of distinct clones in immune cell population
After sampling a subset of cells from a population, the cells may be classified into different types based on next generation sequencing. We are interested in finding the number of different cell types in the original population based on the sequencing results. There are two complications: (1) we don’t observe the cell type of the sample cells directly and we only observe sequenced DNA segments after PCR amplification; and (2) the sequencing process is prone to errors.
Elizabeth Mellins (Stanford Pediatrics) & Guangbo Chen (Immunity Transplant Infection) - How to identify risk factors using an external control group? A case study of sJIA-ILD cohort
The advent of anti-IL1/IL6 biologics transformed the management of systemic juvenile idiopathic arthritis (sJIA), a debilitating early-onset auto-inflammatory condition. However, in recent years, the rheumatology community started to spot cases of interstitial lung disease (ILD) within the sJIA population, a complication rarely seen in previous decades. To define its clinical presentations and identify potential risk factors, we organized a multi-center retrospective study to initiate a comprehensive investigation on the sJIA-ILD. We found that the complication presented several distinctive clinical features, such as acute clubbing (61 % prevalence), unique radiological findings and pulmonary alveolar proteinosis in biopsy (PAP, 62 %).
However, whole-exome sequencing on 20 patients ruled out the conventional congenital PAP in most cases. Thus, the etiology of the disease is not clear, while its mortality cost is high (75% within 6 years). To elucidate on the relationships between the clinical features, we performed a correlation analysis within the sJIA-ILD cohort. We found a history of exposure to anti-IL1/6 is associated with various distinctive clinical features, including PAP pathology.
Meanwhile, the early onset age of sJIA (< 5 years) was strongly associated with pathological findings of PAP in ILD later (OR = 20). When compared to sJIA not developing ILD, sJIA-ILD tended to be significantly younger only in the anti-IL1/6 exposed group but not in the non-exposed group. They also suffer from unusually high frequency of serious adverse reaction to Tocilizumab (40%, >100 times higher than the background). In addition, patients with both sJIA and Down’s Syndrome also have elevated risk for ILD.
The augmented risk of young age by pre-exposure status to anti-IL1/IL6 biologics indicates a potential developmental cause for the disease. In clinical practice, we recommend to routinely monitor potential ILD symptoms (such as digital clubbing and non-resolving respiratory symptoms) among early-onset sJIA (< 5 years old) patients treated with anti-IL1/IL6 biologics, as well as Down Syndrome patients with sJIA.
Bruce Ling (Stanford Surgery) - Analytical challenges: multi-site multi-omics data production for population health
To devise predictive/preemptive big data solutions for population health, we have employed a comprehensive unbiased multi-’omics’ approach, integrating mass spectrometric data production of metabolomics, lipidomics, peptidomics, and proteomics to define the disease associated molecular “portrait” and relative health risk against the population baseline. With the statistical learning of these mass spec data sets, we aim to provide a more technically and bioinformatically tractable, physiologically relevant, chemically comprehensive, and cost effective assessment of multi-factorial non-communicable diseases. However, analytical challenges are obvious when the needs go beyond the qualitative understanding of the underlying biology but to report the quantitative relative/absolute disease risks. In this Data Studio, case studies will be presented and suggestions will be solicited.
Larry Chu, Dominick Zheng & Urvi Gupta (Stanford Anesthesiology, Perioperative and Pain Medicine) - Machine learning approach to screen for breast cancer with thermography
Accurate and early detection of breast cancer and relapse is a critical part of the strategy to reduce the morbidity and mortality associated with it. While some guidelines recommend mammography for screening, the sensitivity, specificity and patient acceptance of mammograms remains less than optimal. Thermography has the potential to become a reliable diagnostic adjunct for breast cancer screening due to recent advances, including the use of machine learning to enhance its diagnostic accuracy. Achanrya’s Support Vector Machine (SVM) model classified normal and malignant breast tissues from a thermogram with 88% accuracy. In this Data Studio, the investigators will identify and seek advice on aspects that need further refinement. Recent advances and suggestions for future work in the field include adding advanced simulation methods, inverse modelling, imaging protocols, and the introduction of artificial neural networks to predict the location and activity of tumours.
Chun-houh Chen, Research Fellow & Director, Institute of Statistical Science, Academia Sinica, Taiwan - Matrix Visualization for (Big) Health Science Data
“It is important to understand what you CAN DO before you learn to measure how WELL you seem to have DONE it” (Exploratory Data Analysis: John Tukey, 1977). Data analysts and statistics practitioners nowadays are facing difficulties in understanding higher and higher dimensional data with more and more complexity while conventional graphics/visualization tools do not answer the needs. It is a more difficult challenge to understand overall structure in big data sets, so good and appropriate Exploratory Data Analysis (EDA) practices are going to play more important roles in understanding what one can do in the big data era.
Matrix Visualization (MV) has been shown to be more efficient than conventional EDA tools such as box plots, scatter plots (with dimension reduction techniques), and parallel coordinates plots for extracting information embedded in moderate to large data sets of binary, continuous, ordinal, and nominal nature. In this study we plan to investigate feasibility of and potential difficulties in applying MV techniques to visualizing and exploring structure in big data: 1) memory/computation (permutation with clustering) of proximity matrices for variables and subject; 2) display of data and proximity matrices for variables and subject. We shall integrate techniques from Hadoop computing environment, image scaling, and symbolic data analysis into the framework of GAP (Generalized Association Plots) to develop an appropriate package for conducting Big Data EDA with visualization. Several international data sets (HCAHPS 2013 Data, MS-DRG 2011 Data) and local data sets (National Health Insurance Data) will be used to demonstrate the bigGAP environment.